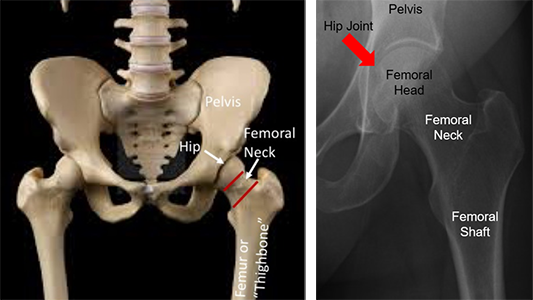
Basic Anatomy
A femoral neck fracture is a type of hip fracture or a broken hip. Your hip joint is made up of two bones: the femur, or "thigh bone," and the pelvis, or "socket." Your hip joint is a ball-in-socket joint that allows you to bend at the top of your leg when walking. Hips that break between the ball and tip of the thigh bone have a femoral neck fracture.
Mechanism and Epidemiology
Femoral neck fractures in young patients typically happen due to a "high-energy" event such as a car accident, motorcycle accident, or dirt bike accident. In these cases, patients younger than 60 years of age with good bone quality are typically considered "young," since their hips break in a different way than older patients with weaker bone.
Initial Treatment
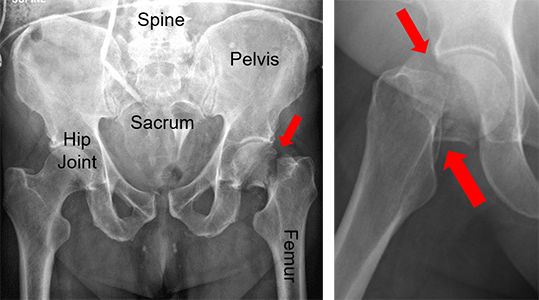
Femoral neck fractures are generally painful and will prevent you from walking. Any movement of your injured extremity typically causes pain. When you break your hip, you are typically taken to an emergency room by ambulance. Once at the hospital, you will get x-rays of your hip and thigh bone. You may need a CT scan of your hip to provide more detail of your broken bone. Your doctor may or may not recommend traction. Traction is a way of gently pulling on your leg until you are able to go to the operating room. This is intended to decrease your pain. Since you cannot walk until your injury is fixed, you will need to be admitted to the hospital for care of this injury. You may also need pain medication.
General Treatment
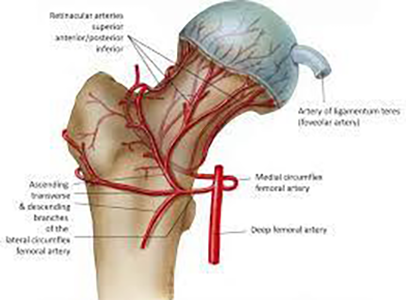
This injury generally requires surgery. Since the blood supply to your hip may have been injured when you broke it, one of the major concerns for this type of fracture is whether it will heal or not. There are a variety of implants that may be used to treat a femoral neck fracture. Which one your surgeon uses depends on the patient and fracture characteristics.



Postoperative Care
After surgery, you will work with physical therapy both in and out of the hospital to rebuild your strength and restore normal walking. How much weight can be placed on your injured leg depends on a number of factors, and it is best to ask your surgeon about this. You likely will be placed on a blood thinner after surgery to prevent blood clots. Blood thinners and early walking are important for preventing blood clots. Several types of pain medication are used for post-operative pain, with the goal to gradually work towards non-narcotic (non-opioid) pain medicine.
You will be discharged from the hospital after a short stay. You may need to spend some time in a rehab facility or skilled nursing facility. You will typically return to see your operating surgeon in the first few weeks after surgery. It is very important that you follow the instructions given you by your treating surgeon.
Long Term
After surgery, you may need an assistive device such as a walker or cane for at least a short period of time after the injury. Physical therapy is usually needed to help you get back to a normal walking motion, and they will also work on muscle strengthening, stretching, and endurance training. It is important to do the exercises learned in therapy at home to make the recovery process as fast as possible.
Complications after femoral neck fracture are infrequent but can occur. These include blood clot, infection, difficulty ambulating, or a limp. Long-term risks include your bone not healing (nonunion) or not healing in the correct position (malunion), prominence of your implants, and arthritis. Long-term complications of joint replacements include dislocations, fracture, and your legs being not equal in length. For some complications further surgery may be necessary.
More Information
---
Justin Haller, MD
Edited by the OTA Patient Education Committee and Dr. Haller (section lead)
All x-rays and pictures taken from the personal collections of Dr. Haller and Christopher Domes, MD