Physical Therapy Videos - Shoulder
What Is It?
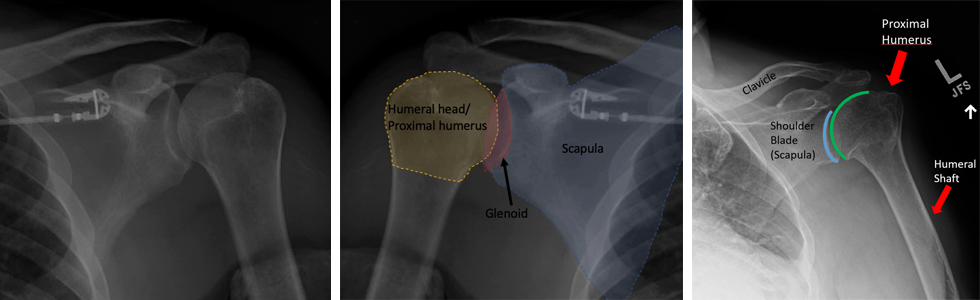
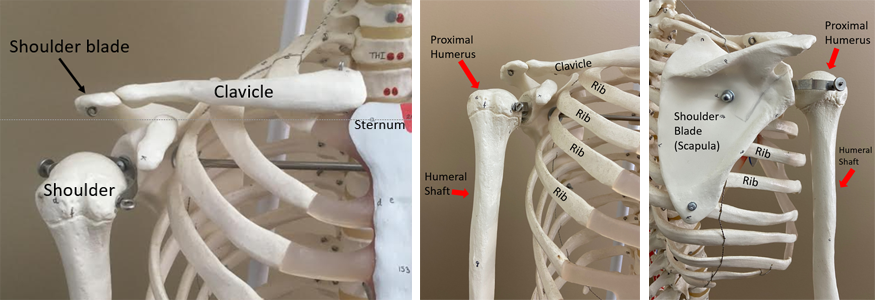
Your shoulder helps you move your arm in many ways. It is made of your upper arm bone (humerus) and your shoulder blade (scapula). The humerus connects to the scapula at a spot called the glenoid. Your shoulder has many muscles around it, like the rotator cuff and deltoid. There are also arteries and nerves that help your arm work.
How It Happens
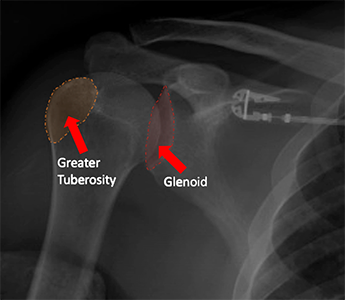
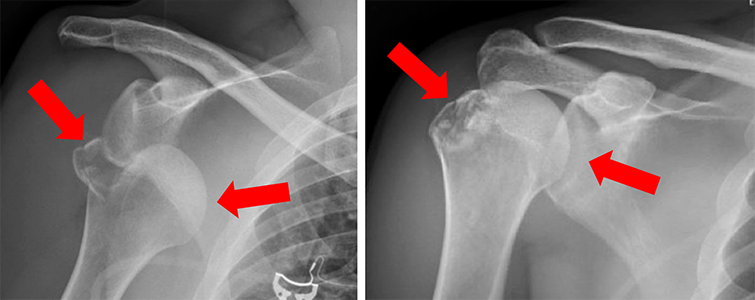
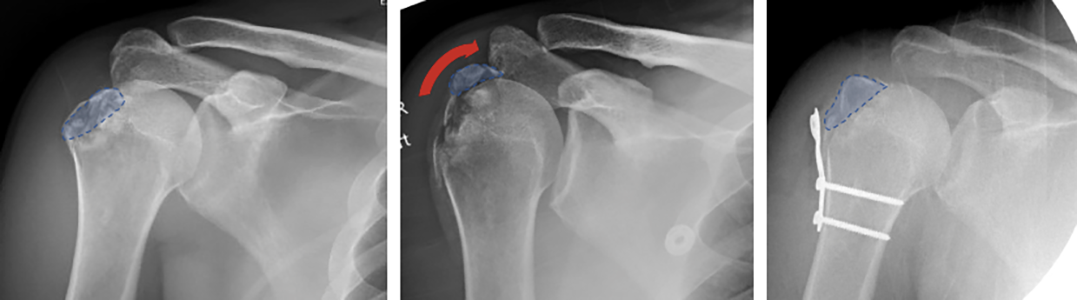
Because the shoulder can move a lot, it can easily come out of place. This is called dislocation. It can happen when your arm twists, gets pulled, or from a fall or hit. When your shoulder comes out of place, the tissues around it can tear. Sometimes, the humerus or glenoid can break. The most common breaks happen in the humerus or glenoid.
First Steps
When your shoulder comes out of place (dislocation), it can hurt and be hard to move. It might feel weak or numb. A doctor will put your shoulder back in place. This is usually done in a hospital with medicines to help with pain. Afterward, they will take an x-ray to check for broken bones. You will be given a sling to hold your arm still and told not to lift anything until you see a bone doctor.
Treatment
Most times, a dislocated shoulder can be treated with a sling. You will work with a therapist to help your shoulder move again and get stronger. Your bone doctor will tell you when you can stop using the sling and use your arm again. If your shoulder also broke when it dislocated, you might need surgery. The type of surgery depends on your injury. It might be done with small cuts or a larger cut with plates, screws, and stitches.
Recovery
If you have surgery, you will need to wear a sling for a while. You will also need to avoid lifting heavy things. A therapist will help you move your shoulder more and get stronger over time. As your bone and tissues heal, moving your shoulder and arm will get easier. It's important to follow your surgeon's instructions about therapy.
Long Term
After a shoulder dislocation, you might have stiffness, weakness, or some pain. Some people feel numb on the outside of their shoulder, which could be permanent. You may not be able to move your shoulder like before. If you have surgery, there can be rare problems like infection or lack of healing, which might need more surgery. If your shoulder came out of place but had no other injuries, it might take four to six weeks to get better. If you have other injuries, it could take much longer to recover, even up to six months. Sometimes, a shoulder can come out of place again. If this happens, your surgeon will talk about your options.
Physical Therapy Videos - Shoulder
More Information
- American Academy of Orthopaedic Surgeons - Shoulder Trauma (Fractures and Dislocations)
- American Academy of Orthopaedic Surgeons - Dislocated Shoulder
---
Sara Putnam, MD
Edited by the OTA Patient Education Committee
X-rays and images from the personal collection of Dr. Putnam and Chris Domes, MD