Physical Therapy Videos - Femur
What Is It?
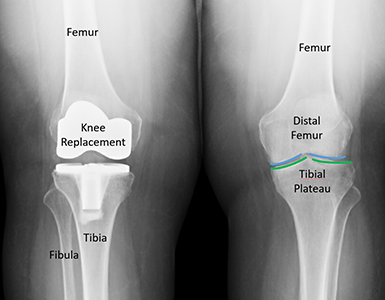
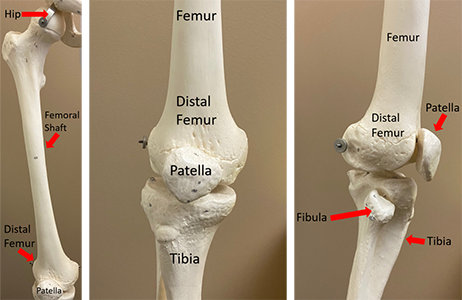
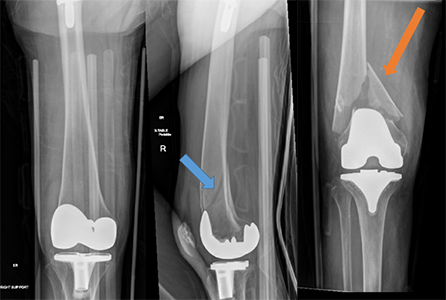
Sometimes, a bone can break around or above a knee replacement. These breaks mostly happen in the thigh bone but can also happen in the top part of the shin bone (tibia). The thigh bone is surrounded by large muscles, which can help the bone heal. However, breaks can be very painful because of muscle cramps. Breaks can also happen between a hip replacement and a knee replacement.


How It Happens
Many knee replacements happen each year, especially in people over 50 years old. These breaks mostly happen because of falls, like falling from a chair or in the shower. Older people might have weaker bones, so even a short fall can cause a break. Breaks can also happen during a joint replacement or in a car accident.
First Steps
A broken thigh bone is a serious injury. You won't be able to put weight on that leg and will need an ambulance to take you to the hospital. In the hospital, you'll get tests to check for other injuries or problems. If you hit your head or can't remember what happened, tell the emergency team. They'll make sure your head, heart, and other body parts are okay.
In the emergency room, your leg might be put in traction, a brace, or a splint to keep it from moving and getting more damaged. You'll likely stay in the hospital and might be moved to a specialized hospital for more care. You'll get more tests, like x-rays and CT scans, for your leg and other body parts.
Treatment
Most of these breaks need surgery. How the surgery is done depends on many things, like where the break is, if it touches the knee replacement parts, and what type of knee replacement you have. Your surgeon will talk to you about the options, which include using a plate with screws or cables, a nail that goes through part of your knee replacement and into your thigh bone, or a new knee replacement that replaces part of your thigh bone.

Recovery
After surgery, you'll have some pain. Your doctors and nurses will help you control it. You might need physical therapy during your hospital stay to help you get better at moving and doing activities. You might need to use a cane, walker, or wheelchair for a while. Some patients need to go to a rehab facility or skilled nursing facility to get stronger.
Long Term
Many people can go back to their normal activities after this injury. But it's important to prevent future falls or injuries. You should talk to your surgeon and primary care doctor about your bone health to help prevent other fractures. Sometimes, the plates, screws, or nails used to fix the break need to be removed with another surgery. Sometimes, the break doesn't heal and needs another surgery to help it heal. Your knee replacement might wear out over time, and you might have stiffness or weakness. Older people might take longer to recover than younger people.
Physical Therapy Videos - Femur
More Information
---
Christopher Domes, MD
Edited by the OTA Patient Education Committee and Justin Haller, MD (section lead)
All x-rays and pictures taken from the personal collection of Dr. Domes