Physical Therapy Videos - Knee
What Is It?
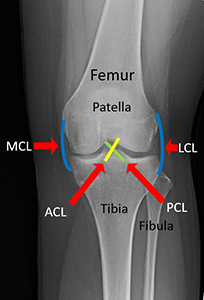
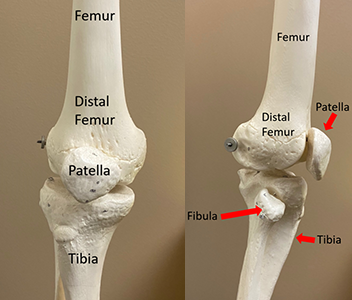
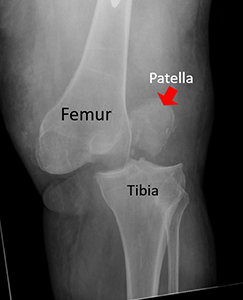
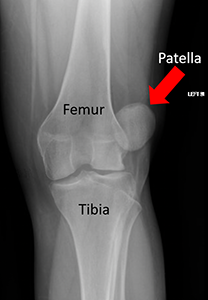
Your knee is a joint between your thigh bone (femur) and lower leg bone (tibia). It has a special bone called the kneecap (patella). Smooth covers called cartilage are at the ends of bones, which let you bend your knee easily. Strong muscles in your thigh help you bend and straighten your knee. Your knee has many ligaments, like ropes, that hold the bones together. Sometimes, the knee dislocates, which means the bones don't line up right.

How It Happens
A dislocation is rare and can happen from car accidents, twisting, falls, or sports injuries.

First Steps
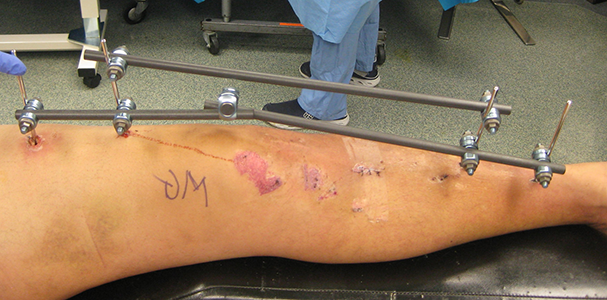
If you have a knee dislocation, it will be painful and hard to move. You need to go to the emergency room. The doctor will check your knee, take x-rays, and put the bones back in place. You might need to wear a brace or have surgery. An external fixator may need to be placed. This is pins and bars in and around the skin to hold the knee in place. The doctor will watch for other problems like blood flow issues or muscle damage. If needed, you may have more tests and surgeries to fix those problems.

Treatment
Knee dislocations are treated by keeping your knee still for a while or having surgery to repair the ligaments. You may need to wear a brace, use crutches, or have a special device (external fixator) to keep the bones in place.

Recovery
Your doctor will decide how long you need a brace or other support. You may need physical therapy to help you move your knee again. It can take a long time to get better. You may need several surgeries to repair the damage. If there is damage to the skin, nerves or blood vessels this may require even more surgeries.
Long Term
Healing from a knee dislocation can take a long time and be hard. Your injured knee might be stiffer and weaker than before. You could get arthritis or have nerve damage. If you have nerve damage this may take over a year to recover. Sometimes nerves do not heal. This may mean you need to use a brace cane or other device. If your blood flow was hurt, it might cause more problems. It is important to follow your doctor's advice to prevent issues. In rare cases, the damage may be so bad that an amputation is needed.
Physical Therapy Videos - Knee
---
Christopher Domes, MD
Edited by the OTA Patient Education Committee
All x-rays and pictures taken from the personal collections of Dr. Domes, Lisa Taitsman, MD, MPH, and Gerald Lang, MD