Physical Therapy Videos - Hip and Pelvis
What Is It?
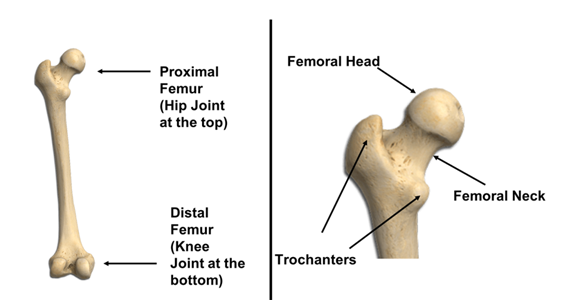
Your hip joint is made up of the top part of your thigh bone (femur) and a socket in your pelvis. The top part of your femur, called the femoral head, is like a ball that fits into the socket. It's covered with cartilage, which helps your hip move smoothly. Muscles are attached to your thigh bone to help you move your leg. The blood vessels to the hip are small and surround the hip joint. If they are damaged with the injury this can cause healing problems.
How It Happens
Hip bone breaks can happen in different situations like sports accidents, car crashes, or motorcycle accidents. These injuries are not common and need special care.
First Steps
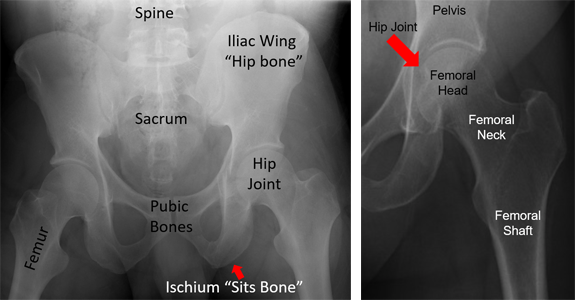
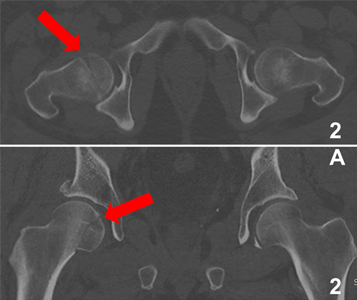
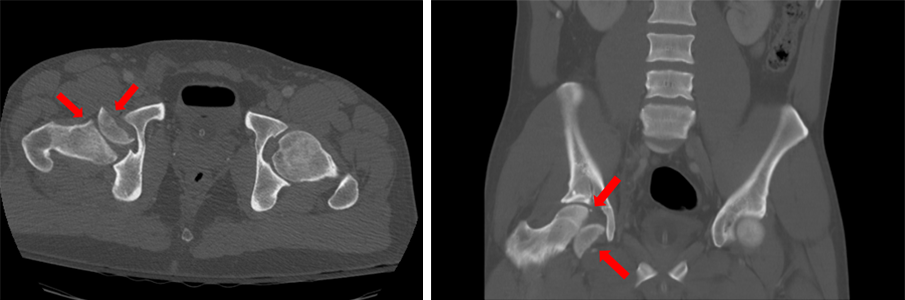
If you break your hip bone, you'll likely feel a lot of pain and won't be able to walk. You'll be taken to an emergency room for tests like x-rays or a CT scan. You might need to stay in the hospital for a while to help with pain and to watch your injury. You might need surgery or be placed in "skeletal traction" to help with pain and fix your broken bone. Skeletal traction is used to keep pressure off the broken bones before they are fixed.
Treatment
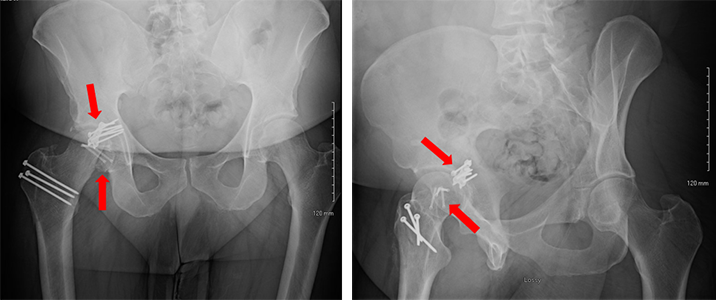
The goal of treatment is to fix the broken part of your hip bone so it's smooth and round again. This can be done with or without surgery, depending on your injury and other factors like your age and overall health. If you need surgery, your doctor will use special tools to fix your broken bone. They may even cut the femur to help see the broken femoral head better. In some cases, if the damage is too severe, you might need a hip replacement.



Recovery
After surgery, it's important to let your bones heal. You'll need to follow your doctor's instructions, which might include not putting weight on your hip and using crutches or a wheelchair. You might work with a physical therapist to help you regain strength and movement. You'll also have regular check-ups to make sure your hip is healing properly.
Long Term
Hip bone breaks are serious injuries because they involve a joint that supports all your weight. You might have complications like infections, blood clots, or long-lasting pain. Sometimes the bones don't heal right or don't heal at all. You might also develop arthritis in your hip joint. These complications might need more treatment, like medications, another surgery, or a hip replacement. Following your doctor's instructions can help lower the risk of complications.
Physical Therapy Videos - Hip and Pelvis
More Information
---
Zachary M. Working, MD
Edited by the OTA Patient Education Committee and Dr Justin Haller (Section lead)
X rays and images from the personal collection of Dr Working, Dr Philip Wolinsky and Dr Chris Domes