Session I - Pelvic Trauma
Intraneural Sciatic Nerve Pressures Relative to the Position of the Hip and Knee
Joseph Borrelli, Jr., MD; Felix Ungacta, MD; Jeffrey Kantor, MD, Washington University School of Medicine, St. Louis, MO
Purpose: This investigation was undertaken to measure the effects of ipsilateral hip and knee position on intraneural pressures of the sciatic nerve.
Methods: Randomly selected fresh elderly cadavers (n=7 ), obtained within 72 hours of death were utilized. Each hip was included in the study if there was no evidence of previous surgery, injury or deformity. Each intact cadaver was placed in the lateral decubitus position on a stainless steel table, and the pelvis stabilized to a custom-manufactured platform with five millimeter Schanz screws. The lower extremity was then flexed and extended maximally at the hip and knee several times to restore flexibility and to assure secure fixation to the platform. The sciatic nerve was exposed via a Kocher-Langenbeck approach; the external rotator muscle attachments were left undisturbed. The femoral attachment of the gluteus maximus muscle was transected to allow exposure of the sciatic nerve, and a single 3-5mm incision was created in the perineurium of the nerve distal to the point of attachment of the gluteus maximus. A 2 mm thick pressure digital transducer (Millar) was placed 4cm into the nerve. The transducer was connected in series with a MacIntosh Powerbook2 and data were collected and saved with LabView 4.0 software. Pressure measurements were taken beginning with the hip in zero degrees of flexion and the knee at 90 degrees (0/90). The hip and knee were then individually moved through a series of positions by a single investigator who was not aware of the pressure measurements. The limb was held at each station for twenty seconds to allow for data collection. The final position was at 90 degrees of hip flexion and the knee fully extended (90/0). Three trials were recorded for each extremity in an identical fashion. Paired t-test and two-tailed paired t-tests were performed for each position to identify differences in intraneural pressures with change in limb position.
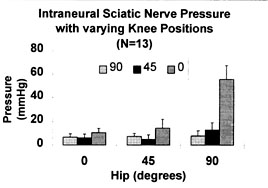
Results: Thirteen of the fourteen hips available were utilized. One hip had undergone a hemi-hip arthroplasty. For convenience, the position of the hip and knee will be presented with the amount of flexion for the hip first and that for the knee second (i.e. 0/90, hip at zero degrees of flexion and the knee flexed to 90 degrees). Average pressures and their standard deviations are provided in mmHg (Table 1). Statistically significant (p=<0.05) increases in the intraneural pressures were measured between position 90/90 and 90/45 (p=0.048) and between 90/45 and 90/0 (p=<0.01). For comparison of results with the knee position held constant and the hip flexed, significant increases were recorded between 45/45 and 90/45 (p=<0.0062), and between 0/0 and 45/0 (0.0006) and between 45/0 and 90/0 (p=<0.01).
Table 1.
Position
0/90
0/45
0/0
45/90
45/45
45/0
90/90
90/45
90/0
Ave.
6.90
7.47
7.89
6.12
4.89
12.84
10.57
14.33
55.65
S.D.
2.53
3.07
3.60
2.36
3.92
7.45
4.28
6.16
11.64
Discussion: Sciatic nerve injury that occurs during open reduction and internal fixation of displaced acetabular fractures is believed to result from traction forces on the nerve or retraction applied directly to the nerve. Somatosensory evoked potential monitoring and electromyographic modalities have been employed in an effort to minimize the incidence of complications. While these measures have positively affected the incidence of this complication, the greatest impact has been realized by maintaining the hip extended and the knee flexed during surgery performed from the posterior approach as recommended by E. Letournel.
The results of this investigation indicate that the intraneural pressures of the sciatic nerve are influenced by the position of the ipsilateral hip and knee. The lowest measured pressures were realized when the hip was flexed less than 45 degrees and the knee flexed to 90 degrees. This position is thought to exert the least amount of strain on the nerve, thereby maximizing the intraneural volume and minimizing intraneural pressure.
The greatest levels of intraneural pressure were noted when the knee was extended from 90 degrees of flexion to 45 degrees while the hip was held in 90 degrees of flexion (90/90 to 90/45), and when the knee was extended from 45 degrees of flexion to 0 degrees (90/45 to 90/90). The increases were statistically significant between each of these stations. When the knee was held in a constant position and the hip was flexed, pressures within the nerve also increased. This was particularly true when station 45/45 was compared to station 90/45 (p=<0.0062), when station 0/0 was compared to 45/0 (p=<0.0006) and station 45/0 was compared to 90/0 (p=<0.01). These data indicate that the redundancy in the nerve (neural and non-neural elements) is taken up by flexing the hip or by extending the knee and that any further increase in stretch on the nerve (either with further knee extension or hip flexion) causes greater increase in intraneural pressure. How this pressure curve will change when the external rotators are released and a sciatic nerve retractor is placed within the lesser sciatic notch remains to be seen. It is possible that the pressure curve will be shifted to the left as the redundancy is taken out of the nerve at an earlier point in this situation.
Significance: 1. Intraneural sciatic nerve pressures are influenced by the position of the ipsilateral hip and knee. 2.) The magnitude of pressure elevation appears to relate to the excursion of the nerve as the linear distance between the greater sciatic notch and the distal aspect of the leg increases. 3. Maintaining the hip in 45 degrees of flexion protects the nerve from significantly increased intraneural pressures. This arc of hip motion may represent a "safe zone" for protecting the nerve from iatrogenic injury during acetabular fracture surgery.