Session III - Hip / Femur
Fri., 10/11/13 Hip/Femur, PAPER #54, 11:13 am OTA 2013
•Fixation of Displaced Femoral Neck Fractures in Young Adults: Fixed-Angle Devices or Pauwel Screws?
C. Max Hoshino, MD; Matthew W. Christian, MD; Robert V. O’Toole, MD;
Theodore T. Manson, MD;
Department of Orthopaedic Surgery, R Adams Cowley Shock Trauma Center,
Baltimore, Maryland, USA
Purpose: Traditional parallel screws have been shown to perform poorly compared to fixed-angle devices for displaced femoral neck fractures. However, many North American trauma surgeons use Pauwel screws that feature a lag screw directed from the greater trochanter inferiorly towards the calcar instead of parallel screws. Our hypothesis was that Pauwel screws would perform as well as fixed-angle devices for these fractures.
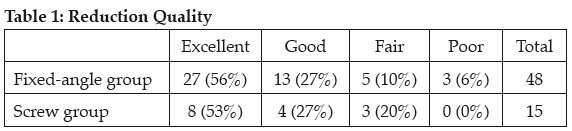
Methods: A retrospective analysis of consecutive femoral neck fractures was performed using our prospectively maintained database. From January 2001 to June 2012, 205 femoral neck fractures in young adults (16-60 years old) were treated with internal fixation at our Level I trauma center. After excluding patients with nondisplaced fractures (72), parallel screw configurations (20), locking plates (8), cephalomedullary nails (2), and <6 month follow-up (41), 2 cohorts were formed. The fixed-angle group consisted of 47 patients (48 hips) that were treated with a side plate and screw/blade device (DHS/DHHS, Synthes), while in the screw group 15 patients (15 hips) were treated with a lag screw placed from the greater trochanter into the inferior neck followed by multiple cancellous screws parallel to the femoral neck. The quality of reduction was judged using the Haidukewych criteria. There were no significant differences between the treatment groups with regard to age, sex, initial displacement, time to surgery, or reduction quality (all P >0.05). An open reduction was performed in 95% of cases resulting in a good-excellent reduction in 83% of cases (Table 1). The average follow-up was 17.2 months.
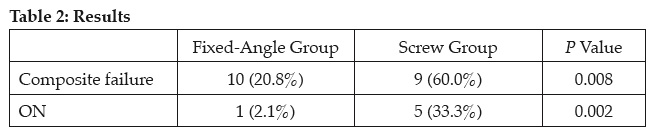
The primary outcome measure was a composite failure metric of a completed or scheduled operation to treat ON (osteonecrosis) or nonunion.
Results: There were significantly more failures in the screw group (60%) compared to the fixed-angle group (21%) (P = 0.008) (Table 2). ON was rare in the fixed-angle group, occurring in 2% of cases versus 33% in the screw group (P = 0.002). Consistent with prior work, good-excellent reductions had a failure rate of 31% compared to 64% with a fair-poor reduction (P = 0.08). The best-case scenario of a good-excellent reduction with a fixed-angle device yielded a success rate of 85%.
Conclusion: Despite the theoretical mechanical advantage of Pauwel screws over parallel screws, this screw configuration still performed poorly compared to fixed-angle devices. In young patients with high-energy femoral neck fractures, lower complication rates are observed with anatomic reduction and fixed-angle devices.
Alphabetical Disclosure Listing
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.