Session I - Polytrauma / Pelvis / Post-Traumatic Reconstruction
Thurs., 10/10/13 Polytrauma/Pelvis/Post-Trauma, PAPER #29, 3:26 pm OTA 2013
Pain and PTSD Following Major Extremity Trauma: Results from the METALS Study
Renan C. Castillo, PhD; Anthony R. Carlini, MS; Ellen J. MacKenzie, PhD;
for the METALS Study Group;
Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, USA
Background/Purpose: Soldiers injured in Iraq and Afghanistan experience significant rates of chronic pain and posttraumatic stress disorder (PTSD), and major limb injuries are a primary cause of disability in this population. However, the extent to which pain and PTSD drive disability among veterans who have experienced major limb injuries is not known. This study was undertaken to assess the burden and co-occurrence of pain and PTSD among service members who sustained a major limb injury while serving in Afghanistan or Iraq, and examine the extent to which these conditions are associated with functional outcomes.
Methods: METALS (Military Extremity Trauma Amputation/Limb Salvage) is a retrospective cohort study of 429 United States service members who sustained major limb injuries (defined as one or more of the following: traumatic amputation, revascularization, bone graft or transport, local or free flap coverage, complete deficit of a major nerve, or compartment syndrome) while serving in Afghanistan or Iraq. Outcomes assessed by telephone interview (mean 38 months postinjury) were: function using the Short Musculoskeletal Functional Assessment (SMFA); PTSD using the PTSD Checklist (PCL) and Diagnostic and Statistical Manual (DSM) criteria; and pain using the Chronic Pain Grade Scale.
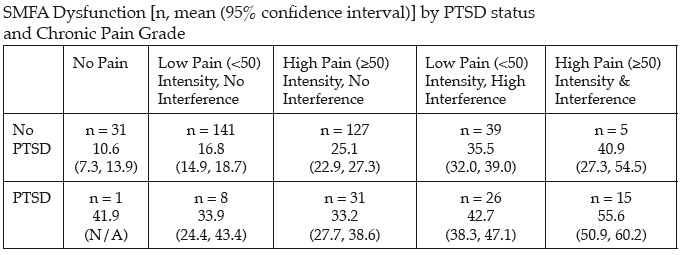
Results: As previously reported, significant long-term pain was observed in this population (mean pain: 49.8 ± 22.8), as well as a high prevalence of PTSD (25% met both the PCL and DSM criteria). As shown in the table below, there was a marked relationship between report of pain and PTSD and functional outcome. The age- and gender-adjusted population norm for SMFA dysfunction is 5.4 ± 9.8 and the proposed minimally clinically important difference (MCID) for this measure is 6. The results suggest METALS patients without pain or PTSD were, on average, about one MCID from age- and gender-adjusted population norms. In contrast, METALS patients with low levels of pain and no PTSD were, on average, two MCIDs from population norms. METALS patients with either greater levels of pain, PTSD, or both, were three to four MCIDs from population norms. Regression analyses adjusted for injury type, age, time to interview, military rank, social support, mild TBI (traumatic brain injury)/concussion, and combat experiences showed large, significant effects for both pain and PTSD on 1-year functional outcomes.
Conclusion: Major limb trauma sustained in the military results in significant long-term pain and PTSD. Overall, the results are consistent with the hypothesis that pain and PTSD are major drivers of disability in this population. The correlational nature of the data does not permit ruling out the alternative hypothesis, that function is driving PTSD and pain. However, prior analyses and theory suggest this alternative hypothesis is less likely.
Alphabetical Disclosure Listing
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.