Sat., 10/6/12 General Interest, PAPER #102, 2:01 pm OTA-2012
Δ Utilization of Two Grading Systems in Determining Risks Associated With Fracture Fixation in Multiply Injured Patients
Nickolas J. Nahm, MD; Heather A. Vallier, MD; Timothy A. Moore, MD;
MetroHealth Medical Center, Cleveland, Ohio, USA
Purpose: Early definitive treatment of femur, pelvis, and acetabulum fractures has been shown to reduce pulmonary complications and mortality in stable patients. Damage control orthopaedics (DCO) is a good option for unstable patients at high risk for systemic complications. A clinical grading system (Pape et al) and the early appropriate care (EAC) protocol have been suggested to characterize high-risk patients and to recommend DCO versus early fixation. This study applies each of these criteria to a cohort of multiply injured patients with femur, pelvis, acetabulum, and/or spine fractures to determine their utility in preventing complications potentially related to early definitive surgery in underresuscitated patients.
Methods: 744 patients with femur (n = 568), pelvis (n = 108), acetabulum (n = 90), and/or thoracolumbar spine (n = 19) fractures treated definitively within 24 hours of injury were reviewed. Patients were assigned a clinical condition based on previously defined clinical grading systems: Table 1 (Pape et al) and Table 2 (EAC). Best condition and worst condition analyses were conducted for the Pape criteria due to inherent ambiguities when applying the criteria. Patients were excluded from analysis of each grading system if they did not have all laboratory tests and vitals of interest within 12 hours of the start of surgery. Outcomes included pneumonia, sepsis, acute respiratory distress syndrome (ARDS), deep vein thrombosis, pulmonary embolism, organ failure, renal failure and mortality.
Results: Best condition analysis of the Pape criteria resulted in 737 stable and 3 borderline patients. A higher rate of renal failure was found in the borderline group (33.3% vs 1.5%, P = 0.048). The worst condition analysis stratified patients into stable (n = 695), borderline (n = 30), unstable (n = 7), and in extremis (n = 8) groups. A higher mortality rate was found in the borderline group compared to the stable group (3.3% vs 0.3%, P = 0.005). More pneumonia (47.5% vs 4.9%, P = 0.006), organ failure (12.5% vs 0.1%, P = 0.023), and deaths (25.0% vs 0.3%, P <0.001) were found in the in extremis group compared to the stable group. By EAC criteria, 104 of 110 patients (94.5%) were resuscitated adequately for early definitive treatment. The other 6 patients, who also received definitive treatment within 24 hours of injury, developed more ARDS (33.3% vs 1.9%, P = 0.014) and renal failure (33.3% vs 1.9%, P = 0.014). No differences were found for other complications.
Conclusion: The Pape criteria differentiate patients at high risk for systemic complications who may benefit from DCO. However, only 8 patients in the worst condition analysis and none in the best condition were in extremis and were at higher risk for complications. One borderline patient and no unstable patients had complications, indicating that more work may be required to clarify the criteria in order to account for all clinical presentations. Furthermore, the use of this complex grading system in the acute resuscitation period requires further study. The EAC protocol provides simple guidelines that effectively distinguish high-risk patients, with less than 2% of lower risk patients having complications after early surgery. Additional study may determine whether the EAC criteria are valid for the spectrum of patient injuries and comorbidities seen at a regional trauma center.
Δ OTA Grant
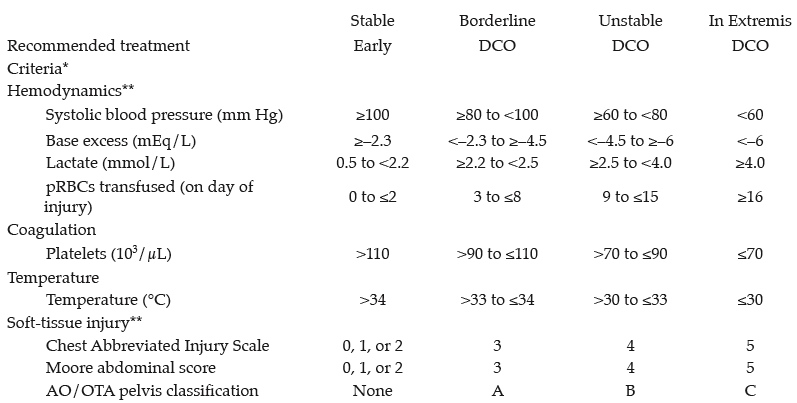
Table 1 Clinical grading criteria (Pape et al)
*At least 3 of 4 major criteria (hemodynamics, coagulation, temperature, or soft-tissue injury) are required to be placed in a clinical grade. If 3 or 4 major criteria are not met, the clinical grade with the 2 major criteria is assigned when possible. If only 1 major criterion is met for each clinical grade, an average clinical grade is determined.
**Best condition analysis places patients in the lowest possible clinical grade for the hemodynamics and
soft-tissue injury major criteria based on the respective subcriteria. Worst condition analysis places patients in the highest clinical grade. All patients in these analyses had at least a platelet value or temperature, at least one hemodynamic subcriterion, and all soft-tissue subcriteria.
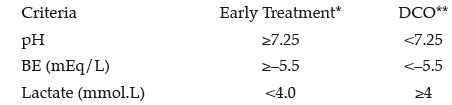
Table 2 Early appropriate care protocol
Alphabetical Disclosure Listing (808K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.