Sat., 10/6/12 Femur/Tibial Fx/Knee Injuries, PAPER #80, 9:27 am OTA-2012
Δ Risk Factors for Reoperation and Mortality Following the Operative Treatment of Tibial Plateau Fractures in Ontario 1996–2009
David Wasserstein, MD, MSc1; Hans J. Kreder, MD, MPH, FRCSC1,2; Michael Paterson, MSc2; Richard J. Jenkinson, MD, FRCSC1;
1Division of Orthopaedic Surgery, Sunnybrook Health Sciences Centre
and University of Toronto, Toronto, Ontario, Canada;
2Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada
Purpose: We previously performed a population-based matched cohort study comparing rates of total knee replacement after operatively treated tibial plateau fractures (AO type 41A-C). The purpose of this study was to identify risks for reoperation (including revision and washout for deep infection) among patient, surgical, and provider factors within the surgical plateau fracture population cohort. Risk factors for early mortality were also examined.
Methods: Administrative datasets from the Province of Ontario were used to identify all patients who underwent operative fixation of the tibial plateau between 1996 and 2009. Patients younger than 16 years, non-Ontario residents, those with bilateral injuries, or who underwent knee replacement or tibial plateau fracture surgery in the 5 years prior to the index event were excluded. Outcomes included infection, revision, amputation, fusion, and hardware removal within 1 year of the index event, and 90-day mortality. Multivariate logistic regression analysis was fit to the data and included patient demographics, surgical (eg, fracture features), and provider (surgeon volume, academic hospital status, time of surgery–overnight and after 5 PM) factors as covariates. Odds ratios (OR) with 95% confidence intervals were calculated.
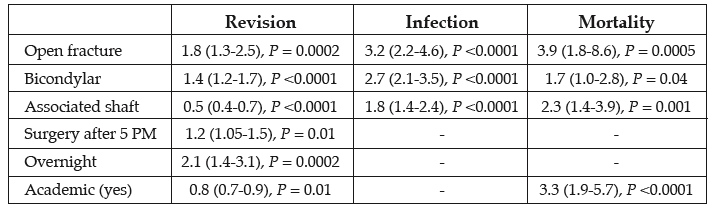
Results: The operative cohort included 8426 patients with a median age 48 years (interquartile range, 37-61) and 51.5% male. Markers of higher-energy injuries such as open fractures, procedures billed as bicondylar, or with an associated tibial shaft fracture increased the risk of reoperation and mortality (see table). Males were also at increased risk of infection (OR 1.7 [1.2-2.2], P = 0.0006). Age each year above the mean increased mortality risk 10% (OR 1.1 [1.09-1.14], P <0.0001). Surgeon volume of procedure did not influence any outcome.
Alphabetical Disclosure Listing (808K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.