Fri., 10/5/12 Pelvis & Acetabulum, PAPER #58, 3:06 pm OTA-2012
Core Muscle Size and Mortality Following Nonoperative Management of Pelvic Fractures
William D. Scheidler, BS; Shaun P. Patel, BS; Sven A. Holcombe, BS2;
Stewart C. Wang, MD, PhD; James A. Goulet, MD;
University of Michigan, Ann Arbor, Michigan, USA
Background/Purpose: The incidence of pelvic fractures in the United States is estimated to be 37 cases per 100,000 person-years. In the geriatric population, 94% of pelvic fractures are low-impact, osteoporotic fractures. One out of every five geriatric patients dies within 1 year of their pelvic fracture. While fracture risk can be estimated through bone densitometry, there are limited data predicting postfracture survival. Core muscle size, a proxy measure of patient frailty, may serve as one such variable to help risk-stratify patients. Specifically, we hypothesized that decreased core muscle size would lead to increased mortality.
Methods: We identified 405 patients undergoing nonoperative management of a pelvic fracture at the University of Michigan Health System between February 2004 and January 2011 who had a CT scan of their abdomen/pelvis within 90 days of their diagnosis. To select for low-impact injuries in an osteoporotic population, we included only females over age 50 and men over age 65 with an ISS <18. Our primary independent variable was core muscle size, defined as the total cross-sectional area of the psoas muscles at the level of the fourth lumbar vertebra (L4), normalized to height to account for body type variance. Our dependent variable of interest was 1-year mortality following the fracture. Bivariate analyses were subsequently performed.
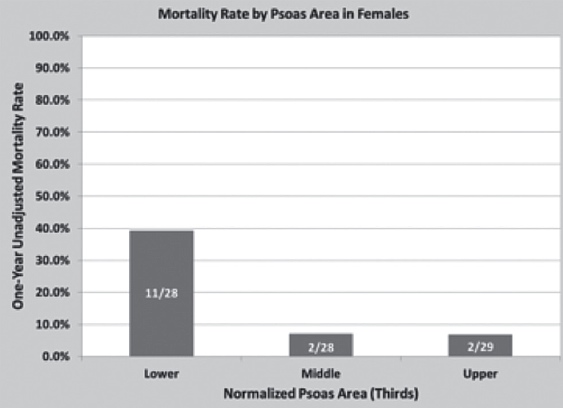
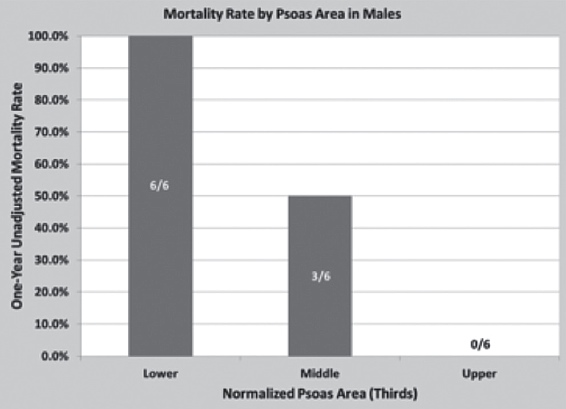
Results: 103 patients met our selection criteria (85 females, 18 males). 24 patients (15 female, 9 male) died within 1 year of their diagnosis (23.3% overall, 17.6% female, 50% male). When stratifying females into thirds by normalized psoas area, the patients in the lower third had a significantly higher 1-year mortality rate compared to patients in the upper third (39.3% vs 6.9%, P = 0.0001). When similarly stratifying males, the patients in the lower third also had a significantly higher 1-year mortality rate compared to patients in the upper third (100.0% vs 0.0%, P = 0.002).
Conclusion: In nonoperatively managed pelvic fractures, our data indicate that decreased core muscle size leads to significantly increased mortality rates. Such objective measures of patient frailty may potentially inform clinical decision-making and improve orthopaedic patient risk stratification.
Alphabetical Disclosure Listing (808K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.