Fri., 10/14/11 Knee, Foot & Ankle, Paper #66, 4:50 pm OTA-2011
Payer Status and Increased Distance Traveled for Fracture Care in a Rural State
William Lack, MD; Julian Carlo, MD; J. Lawrence Marsh, MD;
University of Iowa Hospitals and Clinics, Iowa City, Iowa, USA
Purpose: Orthopaedic patients that require emergent care and have severe injuries are often appropriately referred to rural trauma centers over great distances but similarly patients with less severe injuries that do not require specialized treatment are also referred for care over similar distances. The goal of this study was to assess changes in distance traveled for rural fracture care and how this varies by case type, injury severity, and payer status.
Methods: A retrospective review of the electronic records was performed at a rural Level 1 trauma center. Adults who presented for the operative management of a defined set of orthopaedic injuries between 1990 and 2007 were divided into simple, complex, and emergent categories. Distance traveled to the tertiary care center and ISS were calculated. Case volume and distance traveled for care were compared by injury type, early (1990 to 1997) and late (1998 to 2007) time periods, and by payer status.
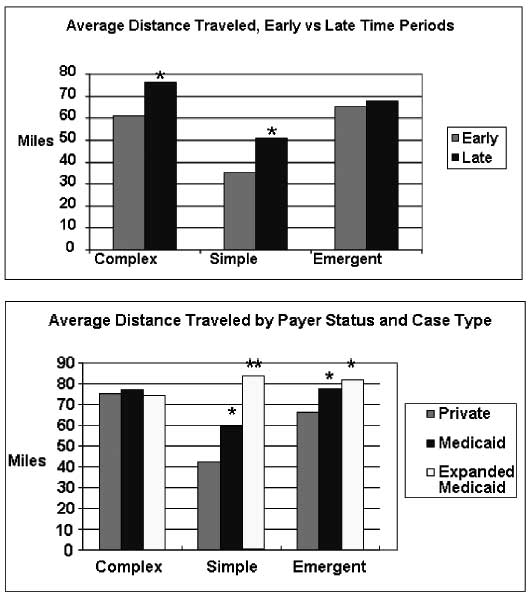
Results: There was an increase in simple, complex, and emergent orthopaedic procedures over time (all P <0.01). Distance traveled increased over time for simple (P = 0.04) and complex (P = 0.03) but not for emergent injuries. Medicaid patients with simple and emergent injuries traveled further than non-Medicaid patients (P < 0.01). Expanded Medicaid patients traveled even further than standard Medicaid patients (P <0.0001) for the care of simple injuries. The ISS was lower for simple than for complex and emergent cases (P <0.001); there was no change in ISS for complex and simple cases over time, while the ISS increased for emergent cases with time (P <0.03). The percentage of patients presenting to the Level 1 trauma center with simple injuries for whom Medicaid was their payer increased from 11.8% to 35.5% (P <0.001).
Conclusions: As the referral of orthopaedic trauma has increased over time, Medicaid patients with simple and emergent injuries have traveled further than patients with other payers and the proportion with simple injuries presenting to the Level 1 trauma center with Medicaid as their payer increased dramatically over time despite no change in injury severity for these patients. Appropriate resources are necessary to handle a rising volume of orthopaedic trauma at regional centers and to ensure that care is equitable. The referral of orthopaedic patients over great distance deserves further study as it affects patient outcomes, cost, and convenience of care.
Alphabetical Disclosure Listing (628K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.