Fri., 10/14/11 Knee, Foot & Ankle, Paper #60, 4:04 pm OTA-2011
Is Fixation of the Medial Malleolus Necessary?
Paul Tornetta, III, MD; Virginia Mooney, MD; Jason Pittman, MD, PhD;
James Daley, MPH; William R. Creevy, MD;
Boston University Medical Center, Boston, Massachusetts, USA
Purpose: The current standard for the treatment of the medial malleolus in bi- and trimalleolar fractures is reduction and fixation. However, multiple clinical and biomechanical studies have demonstrated that while supracollicular fractures (which have the deep deltoid attached) contribute to ankle stability, anterior collicular fractures do not. Intercollicular fractures may add to stability depending on the amount of deep deltoid attached. The most common reason cited for open reduction and internal fixation (ORIF) of the medial malleolus is to avoid the pain of a possible fibrous or nonunion. The purpose of this study is to review the results of a protocol for fixation of the medial malleolus in bi- and trimalleolar fractures based on stability and fragment size and the resultant medial-sided pain and tenderness for both operative and nonoperative treatments.
Methods: Over an 8-year period, we followed a general protocol for fixation of medial malleolar injuries. This included fixation of supracollicular medial malleolar fractures unless there were soft-tissue concerns (13) or if the lateral side was done first and the medial side was well aligned (5). Intercollicular fractures were fixed if they were felt to be large enough to contain some of the deep deltoid ligament or if they were widely displaced after lateral fixation, and anterior collicular fractures were fixed only in active patients or by patient choice. We evaluated these patients specifically looking for medial-sided pain, symptoms, or the need for surgery on the medial side after the definitive treatment. Pain was determined on a 10-point scale. For the purposes of this study, we report any patient who reported >2 (on the 10-point scale) to have medial “pain”.
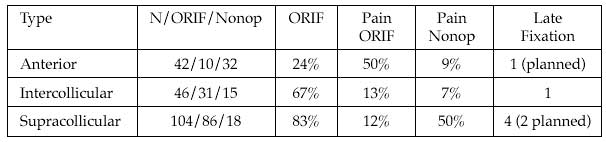
Results: 192 patients, 88 men and 104 women with a mean age of 44.6 years (range, 18-83 years) had bi- or trimalleolar fractures treated with ORIF of the lateral malleolus and either operative or nonoperative management of the medial malleolus. Follow-up averaged 15 months (range, 6-56 months) after their definitive ORIF by either clinic visit or recontact by phone and all patients were followed at a minimum to union and full weight bearing. They were specifically asked about pain on the medial aspect of the ankle and the medial ankle was palpated to determine tenderness. Six patients (4%) who had medial malleolar fixation had symptomatic hardware removed. There were 3 patients who had late ORIF due to symptomatic nonunion (4.5%), of which 2 were in supracollicular patterns. The results are summarized in the table below for each type of medial malleolus fracture:
Conclusions: This series reports on a general protocol of fixation of larger medial malleolar fractures if they are believed to add to ankle stability, or if they are widely displaced after lateral fixation. Smaller malleolar fractures were fixed only in active patients. While pain was more common after fixation than nonoperative treatment of anterior collicular fractures, this was reversed in supracollicular fractures. This study supports fixation of larger fragments to avoid pain and tenderness, but suggests that smaller fragments may be best left unfixed, especially anterior collicular fractures.
Alphabetical Disclosure Listing (628K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.