Thurs., 10/13/11 Basic Science, Paper #37, 4:47 pm OTA-2011
When Does Anterior External Fixation Enhance Construct Stability in Zone II Sacral Fractures? A Biomechanical Evaluation
Christian S. Bromfield, MD1; Erik McDonald, BS2; Michael P. Leslie, DO3;
Jenni M. Buckley, PhD2; Mark A. Lee, MD1; Tania A. Ferguson, MD1;
1University of California, Davis, Sacramento, California, USA;
2University of California, San Francisco, San Francisco, California, USA;
3Yale School of Medicine Orthopaedics and Rehabilitation, New Haven, Connecticut, USA
Purpose: This study was designed to evaluate the biomechanical contribution of anterior external fixation (AEF) to various posterior fixation constructs in both a “reduced” and a “comminuted” (gap) zone II sacral fracture model. Our null hypothesis was that AEF does not increase load to failure over that observed with the posterior fixation alone.
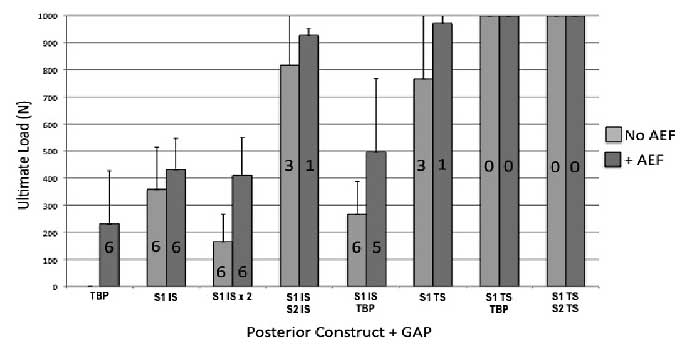
Methods: We simulated a transforaminal sacral fracture with ipsilateral rami fractures (AO/OTA 61-C1.3) in fourth-generation composite epoxy–coated full pelvic models (N = 6). We tested 8 posterior fixation constructs: (1) tension band plate (TBP), (2) single iliosacral (IS) screw at S1, (3) 2 IS screws at S1, (4) IS screws at S1 and S2, (5) IS screw at S1 + TBP, (6) transsacral (TS) screw at S1, (7) TS screw at S1 + TBP, and (8) TS screws at S1 and S2. Each construct was tested with and without AEF (at anterior inferior iliac spine [AIIS]), and with and without posterior fracture gap (simulating a situation in which there is no posterior cortical contact). Load to failure was tested in a single-leg stance model, and displacement was measured by tracking relative motion of the involved hemipelvis with a 3-dimensional motion tracking camera.
Results: The TBP construct was unable to withstand load without an AEF with or without posterior gap. In the setting of posterior cortical contact, addition of AEF contributed to ultimate load to failure only in the setting of single-level IS fixation (S1 IS, S1 IS × 2). The contribution of AEF in the presence of a posterior gap varied by construct. Failures prior to achieving 1000-N load occurred in all constructs except transsacral fixation (S1 TS). AEF enhanced the stability of single-level (S1 only) fixation constructs. When 2-level (S1 and S2) fixation was achieved via IS, TS, or TBP, AEF did not significantly increase the sustainable load.
Conclusions: When used as supplemental fixation, AEF displayed a biomechanical advantage in load to failure when posterior fixation was limited to single-level sacral fixation. The contribution was greatest in the setting of a posterior gap. Transsacral fixation at S1 alone decreased the importance of AEF. With 2 levels of posterior fixation (S1 and S2), AEF made no significant contribution to construct stability. Clinically, this indicates that AEF should be added when safe posterior fixation is limited to S1 IS screws or a TBP alone, but does not improve stability when fixation at both S1 and S2 can be achieved.
Alphabetical Disclosure Listing (628K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.