Sat., 10/16/10 Polytrauma & Femur, Paper #72, 10:58 am OTA-2010
The Military Extremity Trauma Amputation/Limb Salvage (METALS) Study: Comparing Outcomes for Amputation versus Limb Salvage following Major Lower Extremity Trauma
The METALS study group: COL (Ret) William Doukas (WRAMC), COL (Ret) Roman Hayda (BAMC),
Dr. H. Michael Frisch (WRAMC), COL James Ficke (BAMC), LTC Romney Andersen (WRAMC/NNMC),
CDR Michael Mazurek (NMCSD), CDR John Keeling (WRAMC/NNMC),
COL Paul Pasquina (WRAMC), Dr. Harold Wain (WRAMC), Dr. Timothy McHenry (BAMC),
Mr. Anthony Carlini (JHBSPH), Dr. Ellen MacKenzie (JHBSPH)
BAMC - Brooke Army Medical Center, Fort Sam Houston, TX;
JHBSPH - Johns Hopkins Bloomberg School of Public Health, Baltimore, MD;
NMCSD - Naval Medical Center San Diego, San Diego, CA;
NNMC - National Naval Medical Center, Bethesda, MD;
WRAMC - Walter Reed Army Medical Center, Washington, DC
Purpose: This study was undertaken to examine functional outcomes and disability following severe lower extremity trauma sustained as a result of high-energy blast and ordnance- related mechanisms. We hypothesized that outcomes would be similar among those undergoing amputation or limb salvage.
Methods: This is a retrospective cohort study of 298 United States service members who sustained a major lower limb injury while serving in Afghanistan or Iraq. Major limb trauma was defined as having a traumatic amputation or one or more of the following: revascularization, bone graft or bone transport, local or free flap coverage, complete deficit of a major nerve, or complete compartment injury/compartment syndrome. Excluded from this analysis were persons with a major upper limb amputation. Participants were interviewed by telephone (mean 38 months) and medical records abstracted. The Short Musculoskeletal Functional Assessment (SMFA) was used to measure overall function. Additional batteries were used to assess depressive symptoms (Center for Epidemiological Studies Depression Scale [CES-D]), posttraumatic stress (Military PTSD Checklist [PCL]), and chronic pain (the Chronic Pain Grade Scale). Differences in outcomes were compared using regression analysis adjusting for age, time to interview, military rank, presence of a major upper limb injury, social support, and combat experiences.
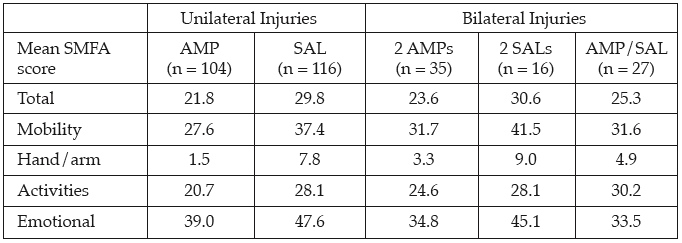
Results: Participants report high levels of disability. 40% have depressive symptoms (CESD ≥16); 20% screen positive for posttraumatic stress (PCL ≥50). One-fifth report pain that interferes with daily activity and 35% were not working, on active duty, or going to school. Mean SMFA scores are shown below for 5 principal groups defined by unilateral versus bilateral injuries and whether the injury resulted in amputation (AMP) or limb salvage (SAL). After adjusting for covariates, patients with at least 1 major AMP had better scores on all domains of the SMFA (P < .001) compared to those without an AMP. There were no significant differences by AMP status in percent with depressive symptoms, posttraumatic stress disorder (PTSD), or pain interference.
Conclusion: Major lower limb trauma sustained in the military results in significant longterm disability. As a group, those undergoing amputation appear to have better functional outcomes than those definitively treated with limb salvage. Further study is needed to determine if differences are related to rehabilitation protocols, ancillary services, or other external factors.
Disclaimer: The views expressed in this presentation are those of the authors and do not reflect the official policy of the Department of the Army, Navy, Department of Defense, or US Government.
Alphabetical Disclosure Listing (292K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.