Fri., 10/15/10 Foot & Ankle, Paper #49, 11:20 am OTA-2010
Treatment of the Stress-Positive Ligamentous SE4 Ankle Fracture: Incidence of Syndesmotic Injury and Clinical Decision Making
Paul Tornetta, III, MD; T. William Axelrad, MD; William R. Creevy, MD;
Boston University Medical Center, Boston, Massachusetts, USA
Background: It has been demonstrated that only one-third of patients with an isolated supination–external rotation (SE)-pattern fibula fracture who present with an aligned mortise have instability on stress examination. Those with no instability are treated without surgery without the risk of displacement. The treatment for the stress-positive (stress+) fracture is more controversial. Additionally, while the incidence of syndesmotic instability in subluxated ligamentous SE4 ankle fractures is reported between 19% and 40%, there is no information regarding the incidence of syndesmotic instability in patients with stress+ SE-type fibula fractures.
Purpose: The purpose of this study is to report on a large series of stress+ isolated SE-type fibula fractures, as regards the ability to gain anatomic union, and to report the rate of syndesmotic instability in the operative cases.
Methods: Over a 9-year period, we treated 99 patients (age 19-76 years; average, 43) with stress+ isolated SE-type fibula fractures to union. All presented with an aligned mortise and were found to have widening of the medial clear space (MCS) with talar subluxation on external rotation stress radiographs with the ankle in neutral position. All radiographs were rereviewed and the MCS measured on the presentation, stress, and final united radiographs. The decision for surgical or nonsurgical management was made by the patient and surgeon after a discussion of the risks and benefits of both. The presumed ability to hold the reduction in a cast was part of the discussion in all cases. Syndesmotic instability for the operative cases was defined as medial widening and talar subluxation on an abduction external rotation stress radiograph after fibular fixation. Syndesmotic fixation was performed for any elicited subluxation.
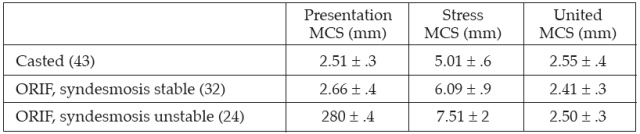
Results: Of the 99 cases, 43 were definitively treated in a cast (6 weeks non–weight bearing, then weight bearing as tolerated in brace and weaned) and 56 were treated operatively. 24 (43%) of the operative cases demonstrated intraoperative syndesmotic instability. The presentation MCS measurements were not different for patients treated with a cast, open reduction and internal fixation (ORIF) fibula only, or ORIF fibula and syndesmosis; however the stress radiograph MCS was statistically different for all groups (P < 0.001) (Table). The casted group had minimal displacement on stress radiograph whereas the operative group had more, with those demonstrating intraoperative syndesmotic instability being greater than those without. No patient healed with any subluxation.
Discussion: Patients with stress+ SE-pattern lateral malleolar fractures are clearly a spectrum of injury. The treatment of these injuries is controversial and outcome has been correlated with initial MCS widening. In this series, clinical judgment resulted in those patients with minimal displacement on the initial stress radiograph being treated successfully nonoperatively and those with greater stress MCS having surgery. Within the surgical group, the incidence of syndesmotic injury is the same as prior reports of ligamentous equivalent SE4 fibular fractures (43%). All patients healed with a well-aligned mortise.
Conclusions: Stress+ SE-pattern fibular fractures with minimal MCS widening on stress radiographs may be treated in a cast to union without displacement. Those with greater displacements (wider MCS) on stress radiographs have an incidence of syndesmotic injury that is the same as patients who presented with subluxation of their ankle and should be sought out.
Alphabetical Disclosure Listing (292K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.