Thurs., 10/14/10 Upper Extremity, Paper #31, 3:31 pm OTA-2010
Corrective Osteotomy for Malunited Fractures of the Distal Radius: Do We Need to Use Bone Graft?
Kagan Ozer, MD; Ayhan Kilic, MD; Kyros Ipaktchi, MD;
University of Colorado, Denver Health Medical Center,
Department of Orthopaedics, Denver, Colorado, USA
Purpose: Malunited fractures of the distal radius are traditionally treated with osteotomy, plating, and bone grafting. The use of bone graft gives additional structural stability and promotes bone healing. Most previous studies on the use of bone grafts at the fracture site were published in an era when volar locking plates were not available. Volar locking plates provide excellent stability and support at the fracture site so that the use of bone graft for the purpose of adding to the structural stability may not be necessary. In this study, we tested the hypothesis that there is no need to use bone graft provided that the contact on the volar cortex is maintained following opening-wedge corrective osteotomy of the distal radius with volar locked plating.
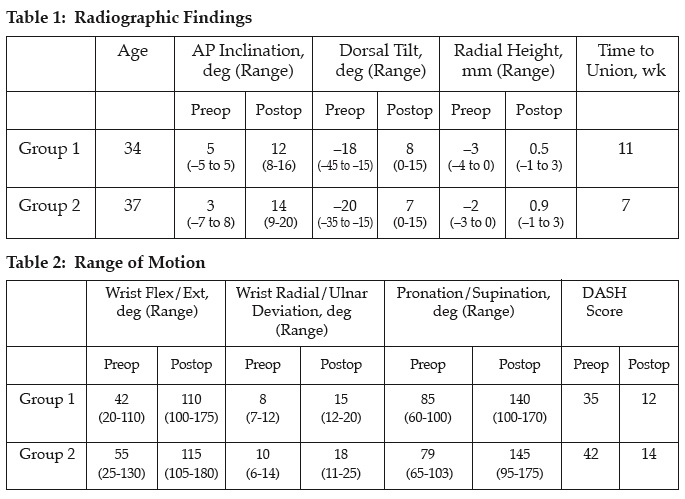
Methods: Two groups of age-matched patients were identified, with dorsally angled malunited extra-articular fractures of the distal radius, who underwent opening-wedge corrective osteotomy with volar locked plating. In group 1 (n = 14), patients refused to receive any form of synthetic graft, allograft, or autograft. In group 2 (n = 14), patients agreed to have allograft (demineralized bone matrix chips) at the osteotomy site. No patients had a body mass index (BMI) above 35 and none of the patients had diabetes.
Results: All patients in both groups had a complete radiographic union at the end of 6 months without hardware failure. Patients in group 1 (without bone graft) had a longer time to union (11 weeks) compared to group 2 (7 weeks) (P < 0.05). Return to work, maintenance of correction at the final follow-up, and Disabilities of the Arm, Shoulder and Hand (DASH) scores showed no statistical difference. One patient had an extensor pollicis longus rupture in group 2 and was treated with a tendon transfer.
Conclusion: In a small cohort of nondiabetic patients with BMIs less than 35, it is possible to achieve complete union following opening-wedge osteotomy of the distal radius without the application of the bone graft, provided that a contact is maintained on the volar aspect of the radius with a locked volar plate. The use of allograft bone chips therefore is not needed. This reduces the overall of the cost of the surgery, eradicates the disease transmission risk associated with the use of bone allograft chips, and finally eliminates the donor-site morbidity seen after autogenous bone grafting.
Alphabetical Disclosure Listing (292K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.