Physical Therapy Videos - Femur
Basic Anatomy
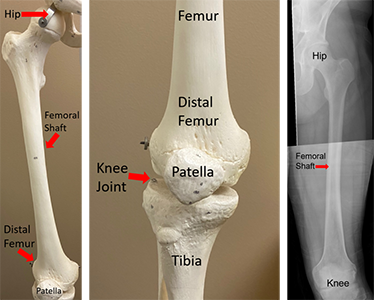
The femur (thigh bone) is the largest bone in your body. The femur is the only bone in the upper portion of your leg, and it is completely covered by your thigh muscles. These include the quadriceps (quads) in the front of your thigh, hamstrings in the back, gluteal muscles, and groin muscles (adductors). Because of this, it’s rare for a broken femur to poke through the skin. The long, middle portion of your femur bone is called the femoral shaft. This section of your bone is about an inch and a half thick. It is also hollow like a piece of pipe. The upper part of your femur is connected to your pelvis through the hip joint, which is shaped like a ball and socket. The lower portion of your femur bone also widens out and connects to your tibia (shin bone) and patella (kneecap) at the knee joint.
Injury and Epidemiology
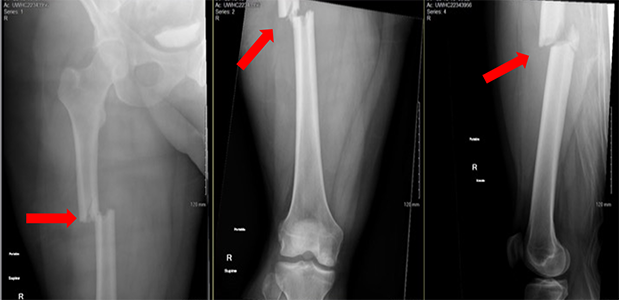
A significant amount of energy is required to cause a femur fracture, most commonly after a car accident, motorcycle accident, fall from a height, or injury from a high-speed activity such as skiing or biking. It’s also common for people with femur fractures to have other injuries. These may include other fractures, internal injuries to the chest, abdomen, or pelvis, and/or injuries to the head or neck. Sometimes these other injuries can be severe or even life-threatening.
Initial Treatment
Femur fractures hurt a lot, and if you break your femur, your leg usually looks “floppy” or deformed. You can’t walk if your femur is broken, so you would typically be brought to the hospital by ambulance. Sometimes paramedics or first responders will place a temporary metal brace, straps, or pillows around your injured leg to stabilize it and make it hurt less. Once you arrive at the hospital, emergency room doctors will carefully examine your whole body to look for other injuries. Several x-rays will be taken, and many times, your doctors will need to get a CT scan of other body parts. This is to look for other injuries and/or to understand your injuries better.
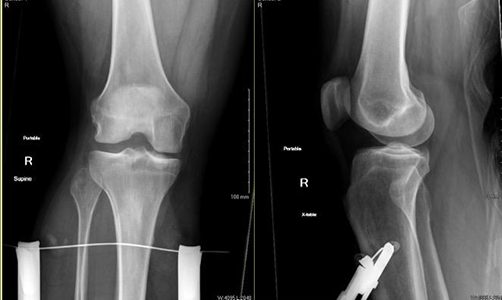
Femur fractures almost always require surgery, but sometimes surgery can’t be done right away. If this is the case, doctors may put something called a "traction pin" into your leg bone above or below your knee and connect this pin to a rope with weights. This is done at the bedside under local numbing medicine. The weights can help to temporarily line up the broken ends of the bone, which can help your leg feel better before surgery.
General Treatment
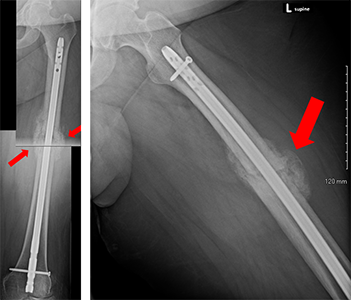
Femur fractures almost always require surgery. The most common way to stabilize or "fix" your broken femur is to place a metal rod, called an "intramedullary nail" ("IM nail" for short) inside the hollow center tube of your femur. Based on factors including other injuries you may have, doctors may choose to put the rod into your femur from the top of the bone (near your hip) or from the bottom of the bone (near your knee). Typically, one or more screws will be placed through holes in the rod above and below the fracture. Because the rod and screws are placed using x-ray guidance, doctors can usually perform the surgery through several small incisions (cuts) in your skin. The rod and screws will stabilize your broken femur, and often you will be allowed to put weight on your injured leg right after surgery. This decision will be made by your surgeon.
If your femur fracture can’t be fixed with a rod, doctors may stabilize the femur with a metal plate and screws placed on the side of the bone. The most common reason for this is the presence of hardware in your femur, such as a hip replacement or knee replacement.

Sometimes, doctors may need to temporarily stabilize your femur fracture with something called an external fixator. This procedure will be performed in the operating room, and involves placing metal pins through the skin and into the bone above and below the fracture. The ends of the pins remain outside your body, and they are connected with bars and clamps, which stabilize the fracture. At some point the external fixator can be removed and your femur may be fixed with a rod or plate and screws.
Postoperative Care
After your femur fracture is fixed, you will probably need to stay in the hospital for a few days. During this time, nurses and therapists will help you begin walking again. Depending on your fracture pattern and how it was fixed, your doctors may place some restrictions on weightbearing. In either case, you will probably need to use crutches or a walker for a while, and you may need to go to a rehabilitation facility or skilled nursing facility. It’s also important to work on bending and straightening your hip and knee joints to avoid stiffness. Other exercises can be done to keep your hip and thigh muscles strong during the recovery process.
You will need to return to your surgeon’s office several times over the weeks and months following surgery. After a few weeks, the stitches or staples used to close the surgical incisions will be removed. X-rays will be taken at different time points to make sure the fracture heals. You may need to do additional physical therapy to build up your strength and balance.
Long Term
Femur fractures fixed surgically usually heal. Your doctors may see signs of healing on x-rays about 6 weeks after surgery, but it normally takes 3 months or more for the femur to fully heal. If your femur doesn’t heal, you may need another surgery to help the bone heal. This surgery would usually include placing additional hardware and may require bone grafting.

Most of the time, once your femur fracture heals, you will be able to return to all of the activities you were able to do before your injury. Long term issues may include stiffness of the knee or hip, soreness at the fracture site, or the feeling that your injured leg isn’t quite as strong as the other side. If your fracture was fixed with a rod, it will probably not need to be removed. Some patients say that their leg feels funny if it gets really cold or if the weather changes quickly. Usually over time they get used to it. If your femur was fixed with a plate, you might have some irritation where the tendons rub over the plate. If these symptoms are bad enough, the plate and screws may need to be removed.
Physical Therapy Videos - Femur
More Information
---
Paul S. Whiting, MD
Edited by the OTA Patient Education Committee and Justin Haller, MD (section lead)
All x-rays and pictures taken from the personal collection of Dr. Whiting and Christopher Domes, MD