OTA 1997 Posters - Tibia Fractures
*A Biomechanical Analysis of Internal Fixation of Complex Tibial Plateau Fractures
Daniel S. Horwitz, MD, Kent N. Bachus, PhD, Christopher L. Peters, MD, David Nilson
Salt Lake City, Utah, USA
Purpose: Over the past decade, the use of external fixation with a ring fixator has increased for the treatment of complex tibial plateau fractures, with or without metaphyseal diaphyseal disassociation. These fractures were previously addressed with medial and lateral buttress plating, the so-called "dead bone sandwich," a technique which has largely been abandoned due to concerns about excessive soft tissue, wound, and infectious complications. We have experienced multiple postoperative complications following the use of the ring fixators for complex tibial plateau fractures, including two infected total knee arthroplasties implanted up to 18-months post-fixation and loss of fixation. We have therefore begun using lateral buttress plates with an anteromedial 3.5 reconstruction antiglide plate for many Schatzker V and VI fractures in our middle-aged population who are at risk for early degenerative joint disease and would be candidates for joint arthroplasty. We believe this provides adequate stability with minimal medial soft tissue stripping. Our goal in this study was to compare the medial stability of the classic dual buttress plating to a single lateral buttress and the newer technique of lateral buttress with a medial antiglide plate.
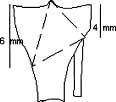
Methods: A series of six cadaveric proximal tibias was osteotomized to simulate a bicondylar tibial plateau fracture with metaphyseal diaphyseal disassociation. These cuts were made to maximize vertical instability (See diagram). Six tibias then underwent ramp loading of 500N to the medial plateau, first with the lateral buttress plate then followed by the addition of a medial buttress or antiglide reconstruction plate, in alternating fashion. Displacement of the medial plateau was measured using the OptoTRAK® measuring system. Following the ramp loads, six specimens in each plate configuration were cyclically loaded with 500N at 5HZ to 10,000 cycles. Displacement of the medial plateau was again measured using the OptoTRAK®.
Results: Displacement of the medial plateau for ramp loads averaged 1.6mm with a lateral buttress plate alone, 0.7mm with a lateral buttress/medial antiglide construct, and 0.6mm with a lateral/medial buttress construct. The cyclically loaded constructs showed medial displacement as follows: Lateral buttress - 5.5mm, lateral buttress/ medial antiglide - 0.8mm, and !ateral/medial buttress - 0.3mm. For both types of loading, the lateral buttress plate provided significantly less stability than either type of medial fixation (p<0.05). We are unable to show a significant difference between the two medial plate constructs.
|
Discussion: The classic AO construct of dual buttress plating has fallen into disfavor largely because of soft tissue, wound, and infectious complications, presumably from massive soft tissue stripping of bone. The ring external fixator, however, is not without its own infectious and mechanical complications. We have therefore compared a different technique of medial plating which we believe offers all the advantages of dual buttress plating while minimizing the soft-tissue stripping necessary for classic dual plating. Our biomechanical testing shows that the medial antiglide construct compares well with the classic plating technique in this cadaveric model of a highly unstable plateau fracture.
Conclusion: The clinical application of ORIF with a medial antiglide plate may offer significant advantages over ring external fixation for Schatzker type V and VI fractures, especially in the middle-aged patient who may require early total knee replacement.