OTA 1997 Posters - Hip Fractures
Optimal Side Plate Fixation for Unstable Trochanteric Hip Fractures
Edward H. Yian, MD, Indraneel Banerji, MD, Larry S. Matthews, MD
University Hospitals, Ann Arbor, Michigan, USA
Purpose: An orthopaedic surgeon must decide how many side plate screws to use when treating an unstable trochanteric hip fracture. This study investigated the minimum cortical bone screw quantity needed for optimal tensile force distribution and fixation of the side plate to the femoral shaft.
Methods: A cortical saw bone model, a steel pipe model, and ten human cadaveric specimens were used. Unstable four-part trochanteric fractures (31-A2.2) were created and specifically designed to prevent medial or posterior bone buttressing. Fractures were stabilized with 120 mm sliding telecoping lag screws and six-hole classic hip screw stainless steel side plates (Smith & Nephew Richards) with 4.5 mm stainless steel cortical bone screws. They were inserted with a torque limiting screwdriver at 3.00 newton-meters. Screw tensions were determined by a 4.5 mm cortical bone screw fitted with a strain gauge instrumented load cell. The femoral shaft was positioned in a fixture at 80 degrees from the horizontal throughout all testing. A vitallium cup lined with neoprene was placed over the femoral head to assure an even distribution of compressive loading. Absolute tension changes were recorded at all cortical bone screw positions when 1334.4 newtons vertical load was quasistatically applied at the femoral head. Decreases in tension, denoted protection, experienced by all previously inserted screws when an additional screw was applied, were also recorded. A mixed model analysis of variance was performed on our data to assess statistical significance.
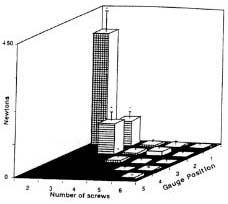
Results: Testing with one bone screw in place produced screw tensile forces up to 1681 N in the steel pipe model, 480.4 N in the saw bone model, and 471.0 N in the human model. With two bone screws in place, a 1570.1, 440.4, and 328.7±96.1 N decrease in tension (p<.001) was noted on screw #1 for the steel pipe, saw bone and human models, respectively (see fig. 1). Protection offered by a third screw on previous screws were 787.3 newtons in the steel pipe model, 71.2 newtons in the sawbone model and 158.4 newtons in the human cadaveric model (p<.005) (see fig. 1). Further distal bone screw placements did not decrease tension in previous screws by more than eleven newtons in each model.
|
Fig 1. Protection of last screw by one additional screw placed distally in human model. Error bars indicate standard deviations. Asterisk indicates statistical significance (p<005). |
Discussion: The results suggest that in a human model, 3 cortical bone screws provide optimal distribution of tensile forces. Forces seen in the steel pipe model were significantly higher than in the other two because of its rigid structure. The human model tested similar to the sawbone model, with force dissipation most likely from elastic deformation. Limitations of the study include the heterogeneous nature of human cortical bone density and thickness, failure to perform cyclical testing, and exclusion of screw bending moment measurements.
Conclusion: This study suggests that three cortical bone screws provide an adequate amount of support needed to prevent side plate displacement from the femoral shaft.