OTA 1997 Posters - Scientific Basis for Fracture Care
*Computed Radiography and Ultrasound as Non-Invasive Predictor of Bone Regenerate Stiffness in Distraction Osteogenesis
Stefan Kolbeck, MD, Hermann Bail, MD, Andreas Weiler, MD, Michael Raschke, MD, Prof. Norbert P. Haas, MD
Trauma and Reconstructive Surgery, Virchow Clinic, Humboldt University Berlin, Germany
Purpose: Advanced management in distraction osteogenesis requires a quantitative estimation of the healing status in order to customize weight bearing and to identify healing failures. Quantitative computed tomography (QCT) is considered as the non-invasive method with the strongest prediction power for torsional stiffness of healing tibial fractures in distracted tibiae (1). Ultrasound (US) attenuation is introduced as an alternative method of measuring skeletal status and recommended as the standard for clinical monitoring in the early phase of limb lengthening (2). X-ray evaluations as the current standard monitoring method of bone healing, have been shown to fail as quantitative predictors of bone healing processes (3). A new technique in projection radiography the computed radiography (CR) with improved image processing and advanced differentiation of tissue densities, raising the possibility of quantitative assessment of bone density and related mechanical properties (4). However, to our knowledge no comparisons between ultrasound data or CR measurements and strength of healing bone tissue have been performed. Our research question was whether torsional strength of the distraction zone can be predicted using CR measurements or analysis of ultrasound data.
Materials and Methods: Tibiae of 30 adult Yucatan minipigs which were part of a drug study were osteotomized, stabilized by an external fixator and, after a latency period of 5 days, distracted 2 mm / day for 10 days. A 10 day consolidation phase followed. Seven ultrasound examinations and CR measurements were carried out during the consolidation period. Using specially adapted cuffs, ultrasound measurements were carried out with a 7.5 MHz linear array transducer at the identical topographic location of the medial tibia. Images were acquired via a video capture card and the penetration depth of the ultrasonic beam was analyzed using an image analysis system. CR measurements were conducted using a special frame to maintain standardized exposure conditions (X-ray source - object distance: 100 cm; 66 kV; 2.5 mAs). An aluminum phantom with 10 steps ranging from 2 to 20 mm was positioned on the same area of every CR-screen. The CR-screens were digitized and transferred to an image work station (Digiscan2", Siemens AG, Munich, Germany). The density values of the step were approximated by a square regression curve (r2 > 0.998) and from this data equal regions of the distraction zone were measured and transformed into so-called equivalent aluminum thickness (EAT). 25 days after surgery the animals were sacrificed. The tibiae were imaged using high resolution computed tomography with 2 mm thick sagittal slices at 1 mm intervals. A hydroxyapatite phantom was included to determine a linear relation between attenuation and bone density. The tibiae were tested to failure in torsion using a material testing machine. Linear regressions were performed between ultrasonic beam penetration depth, the EAT of the distraction zone (measurements at the day before sacrifice) and QCT-calculated bone mineral density (BMD), each as independent variables, and torsional stiffness as the dependent variable. Four animals were removed from the study due to bone infection or surgery failure and data of 2 animals were lost due to test machine failure. In two cases ultrasound measurement data were rejected because of evaluating measurement setup.
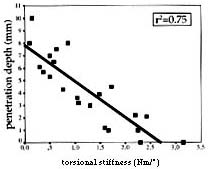
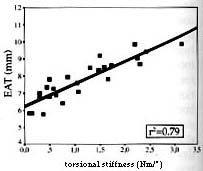
Results: Ultrasound beam penetration depth decreased and CR density of the distraction zone increased constantly as the consolidation period progressed. Torsional stiffness of distracted tibiae (n = 24) ranged from 0.1 to 3.15 Nm/°. The coefficient of determination (r2) was 0.75 for the regression between torsional stiffness and ultrasound beam penetration depth (p < 0.001) (Fig.1) and 0.79 for the regression between torsional stiffness and CR density (p<0.001) (Fig.2) (measurements at the day before sacrifice). The regression between QCT-determined BMD (measurement after sacrifice) and torsional stiffness (p < 0.001) was also 0.79.
Discussion: The correlation between QCT and stiffness is comparable to that reported in former investigations and demonstrates that QCT is useful for the quantification of consolidation in distraction osteogenesis. In our study ultrasound beam penetration depth and CR density measurements were also highly correlated with torsional stiffness. In addition, the visibility of consolidation progress made possible by daily ultrasound investigation suggests that this may provide a sensitive method for detecting early healing status. Due to its wide exposure latitude with a linear signaldynamic, also CR measurements allow to assess early healing stages where conventional X-rays fail and can provide a predictor of bone regenerate stiffness in distraction osteogenesis.
Conclusion: Our results suggest that ultrasound and CR measurements are good predictors, comparable with QCT, of bone regenerate torsional strength during the consolidation period of distraction osteogenesis.
|
|
| Fig. 1: Correlation between ultrasound beam penetration depth and torsional stiffness | Fig. 2: Correlation between EAT of CR measurements and torsional stiffness |
1 Harp et al., Noninvasive Determination of Bone Stiffness for Distraction Osteogenesis by Quantitative Computed Tomography Scans. Clin. Orthop., 301: 42-48 (1994)
2 Hughes et al., Imaging in Bone Lengthening. Clin. Orthop, 308: 50-53 (1994)
3 Panjabi et al., Correlations of radiographic analysis of healing fractures with strength: A statistical analysis of experimental osteotomies. JOR 3:212 -218 (1985)
4 Murphey et al., Computed Radiography in Musculoskeletal Imaging: State of the Art. AJR 158:19-27 (1991).
This work was supported by Novo Nordisk A/S, Gentofte, Denmark