OTA 2013 Posters
Scientific Poster #18 Geriatric OTA 2013
Comparison of Lateral Locked Plating With Additional Distal Fixation and Antiglide Plating for Fixation of Distal Fibular Fractures in Osteoporotic Bone
Robert J. Wetzel, MD1; Neel P. Jain, MD2; Paul J. Switaj, MD1; Brian M. Weatherford, MD1; Mahesh Polavarapu, BS1; Yupeng Ren, PhD3; Xin Guo, MS3; Li-Qun Zhang, PhD1,3;
Bradley R. Merk, MD1; authors received an educational grant for implants and cadavers
from Stryker;
1Department of Orthopaedic Surgery, Northwestern University, Chicago, Illinois, USA;
2Department of Orthopaedic Surgery, Franciscan Alliance, Michigan City, Indiana, USA;
3Rehabilitation Institute of Chicago, Chicago, Illinois, USA
Purpose: Antiglide plating has been described as the biomechanically strongest construct for fixation of distal fibula fractures in osteoporotic bone. The purpose of this study is to compare lateral periarticular distal fibula locked plating to antiglide plating in the setting of an osteoporotic, unstable distal fibula fracture.
Methods: AO/OTA 44-B2 distal fibula fractures were created in 16 paired cadaveric ankles. The bone mineral density (BMD) was determined. The fractures were fixed with a lateral locking plate and an independent lag screw or an antiglide plate with a lag screw through the plate. With the ankle loaded in the axial plane and unconstrained in the coronal and sagittal planes, the specimens underwent stiffness, cyclic loading, and load-to-failure testing. The energy absorbed until failure, torque to failure, construct stiffness, angle at failure, and energy at failure were recorded.
Results: The BMD was not significantly different between the two treatment groups (P = 0.50). Two of the lateral locking plate constructs and four of the antiglide plate constructs failed during cyclical loading. The energy absorbed to failure of the lateral locking construct (29,515 ± 11,958 Nm-deg) was greater than the antiglide construct (24,968 ± 13,190 Nm-deg) (P = 0.03). The lateral locking construct had a higher torque to failure (P = 0.02) and construct stiffness (P = 0.04). The angle at failure trended to be greater for the lateral locking construct (P = 0.07).
Conclusion: The distal fibula periarticular locking plate is biomechanically stronger than a nonlocking one-third tubular plate applied in antiglide fashion for the treatment of AO/OTA 44-B2 osteoporotic distal fibula fractures.
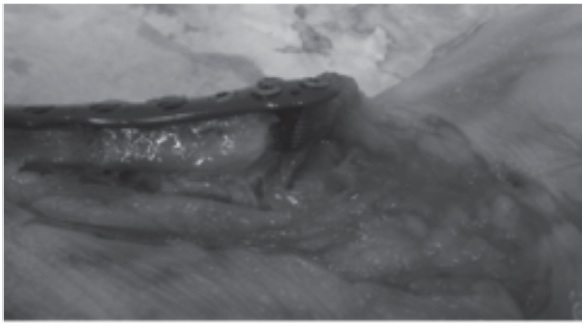
Figure 1: Locking plate failure through catastrophic distal cutout.
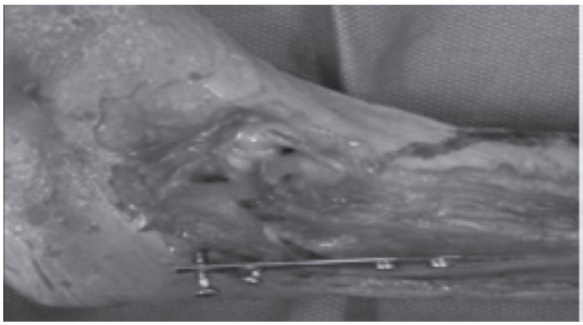
Figure 2: Antiglide plate failure through sequential screw loosening.
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.