OTA 2012 Posters
Scientific Poster #24 Hip/Femur OTA-2012
New Camera-Free Fluorobased Navigation System for Accurate Lag Screw Positioning: Comparison of Conventional Versus Navigated Postoperative Outcome
Rainer H. Burgkart, MD, PhD1; Heiko Gottschling, PhD Inf1; Manuel Schroeder, Dipl Inf1;
Nils Reimers, Dipl Ing2; Heye Janssen3; Arndt P. Schulz, MD, PhD, MRCS3;
1Clinic for Orthopaedics and Traumatology, Technische Universität München,
München, Germany;
2Stryker Osteosynthesis, Schönkirchen, Germany;
3Department Trauma & Orthopaedics, University Hospital Lübeck, Lübeck Germany
Purpose: Outcome of pertrochanteric fracture treatment is essentially dependent on the positioning of the hip screw in the femoral head. Well-established standards indicate the best outcomes are related to a center-center position in the head and a tip-apex distance (TAD) of <25 mm. The goal of this study was to compare the accuracy of the conventional technique with a new camera-free navigated lag screw positioning using TAD and additionally a three-dimensional (3D) inverse reconstruction method (IRM) visualizing the femur head sphere and lag screw in 3D for the 3D distance between tip-head surface in the screw axis (TSD).
Methods: The study is based on the first 12 consecutive patients (median age 84 years, interquartile range [QR] 28 years) treated with a Gamma3 Nail using a new camera-free navigation system compared to 12 patients (median age 86.5 years, IQR 13 years) conventionally treated. Both groups were stratified regarding age (P = 0.897), sex (P = 1.000), and body mass index (P = 0.160). All patients had pertrochanteric fractures and were operated only by experienced surgeons. For supporting the lag screw implantation, the camera-free navigation system visualizes for the surgeon a virtual 3D model of the lag screw and the femur head surface accurately projected in both standard fluoroimages (AP + lateral) according to the position of the targeting arm (Figure 1a).
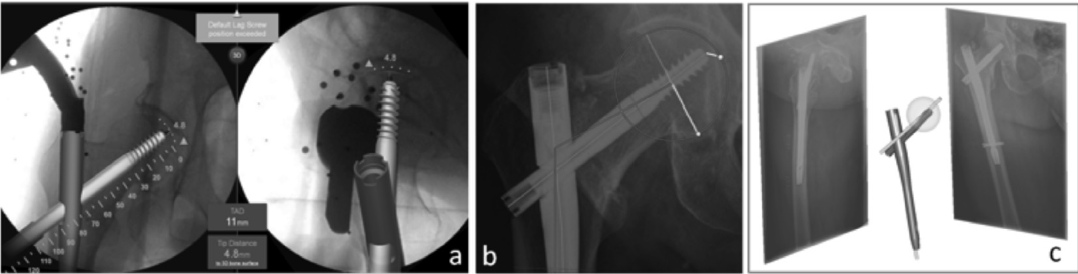
Figure 1. a, the camera-free navigation system provides a projected 3D model of implant and femur head surface;
b, measurements of TAD and Parker´s quotient;
c, inverse 3D reconstruction of implant and femur features (head, CCD, etc) from two
standard x-rays as basis for all 3D measurements.
Therefore the surgeon can directly plan in 3D the type of nail (CCD [caput-collumn-diaphysis] angle), length, and position of the lag screw. Because of a calibration disc mounted to the C-arm, standard C-arms just as conventional surgical tools can be used. To analyze the TAD (Figure 1b) and—also in the conventional group—the 3D position of the lag screw in regard to the 3D femoral head surface a software based IRM was used and corrected for magnification. The IRM application utilizes the known accurate implant dimensions in both radiographic projections at the time of surgery (Figure 1c). For statistical analysis the Wilcoxon test and Fisher exact test (P <0.05) were used.
Results: The median TAD of the conventionally treated group (CG) was 23.8 mm (IQR 7.2, range 17.7-35.5) and thus significantly higher than in the navigated group (NG) with a median TAD of 16.8 mm (IQR 4.4, range 10.1-32.7) (P = 0.002). The known critical TAD value of 25 mm or higher was found in 4 patients of CG due to substantial eccentric screw positions and only in 1 patient of NG with an accurate central screw position, but a 16-mm too short screw. The Parker´s quotient as a measure of the lag screw axis to the head center was in the anterior-posterior direction with 8% (range, 2%-23%) deviation from the optimal 50% in CG, significantly higher compared to 2% in NG (range, 0-11%) (P <0.003). For the superior-inferior direction both groups had equal, very central positions. Finally the 3D evaluation of the tip to head surface (TSD) affirmed the two-dimensional results. The median TSD of CG was 9.2 mm and thus significantly higher than in the NG with 5.7 mm (P <0.005).
Conclusion: To prevent cut-out of sliding hip screws, the most important surgical aim must be an optimal central position of the lag screw with a minimal TAD value. The present study could demonstrate that with a new camera-free navigation system, a higher rate of central positions of the lag screw with significant smaller TAD values compared to the conventional technique can be achieved. With the supporting device, only 1 TAD value was over the critical 25-mm level compared to 4 in the conventional group. Besides the two-dimensional x-ray evaluation, the implemented 3D analyzing tool (IRM) could demonstrate the optimized lag screw positions in the navigated group also 3D with a significantly shorter TSD in the navigated group. Although larger cohorts have to be analyzed, these first results of the new navigation system are already very promising and the new system can be in the future an additional support for surgeons minimizing the cut-out risk by optimized lag screw positioning.
Alphabetical Disclosure Listing (808K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.