Basic Science Focus Forum
Wed., 10/12/11 BSFF: Biomechanics, Paper #3, 9:12 am OTA-2011
Use of Acute Shortening Versus Bridging Plate for Highly Comminuted OTA 21-B1.3(1) Unreconstructable Olecranon Fractures
Akira Yamamoto, MD; Meir Marmor, MD; David Friedberg, MD; Erik McDonald, BS; Eric Meinberg, MD;
University of California, San Francisco, California, USA
Purpose: Highly comminuted unreconstructable olecranon fractures can be treated by excision of the comminuted fragments and acute shortening (AS) of the olecranon or by bridging the comminution with a bridging plate (BP) construct. Biomechanical studies have shown that a significant portion of the olecranon can be excised without compromising elbow joint stability; however, with loss of elbow flexion (EF). Use of a BP may avoid loss of EF; however, there is a paucity of data studying the critical fracture gap at which BP may create an unstable elbow joint. Our hypothesis was that there is a critical fracture gap at which use of a BP will create an unstable elbow joint necessitating use of AS to stabilize the elbow joint.
Methods: Eight cadaveric elbow specimens were used for testing. A standard posterior approach to the olecranon was performed preserving the medial and lateral collateral ligaments and the extensor mechanism. A transverse osteotomy to generate a 2-mm joint gap (JG) in the center of the sigmoid notch, simulating a highly comminuted segment, was created using an oscillating saw. The JG was increased by 2-mm increments up to the point where the olecranon was not amenable to BP. After each osteotomy, the olecranon was fixed using a BP construct (4-hole nonlocking olecranon plate) and then by performing AS and lag screw fixation (3.5-mm screw and washer). Gross stability (joint opening) and range of motion were assessed using C-arm imaging after performing BP and AS at each JG.
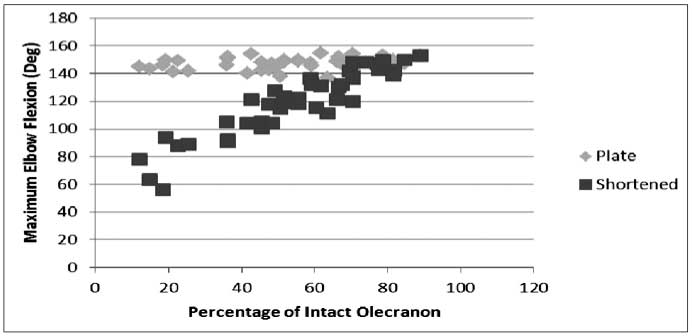
Results: The elbows remained stable after both BP and AS at all JGs with the maximum 88% comminution of the articular surface. Average initial extension was 0° with no change after simulated fracture in both BP and AS. Average initial EF was 146° ± 8 °. Maximal JG (comminution) obtained before BP was unfeasible due to inadequate bony fixation (83% ± 5%). At all JGs for BP, EF was 145° ± 9°. For AS, at 20-40% JG, EF was 137° ± 14°; at 40-60% JG, EF was 117° ± 12°; and at >60% JG, EF was 83° ± 16° (Figure 1).
Conclusion: In highly comminuted unreconstructable olecranon fractures (up to 88% of joint), use of a BP as opposed to AS of the olecranon can maintain full elbow range of motion without compromising joint stability or creating subluxation of the joint. Increasing fracture gap in AS results in a linear decrease in elbow flexion.
Figure 1. Scatterplot graph showing decreasing maximum EF with increasing olecranon comminution in the AS group.
Alphabetical Disclosure Listing (628K PDF)
• The FDA has not cleared this drug and/or medical device for the use described in this presentation (i.e., the drug or medical device is being discussed for an “off label” use). ◆FDA information not available at time of printing. Δ OTA Grant.