OTA 2004 Posters
A Modified Judet Approach to the Scapula
Purpose: We describe an approach for exposure of a displaced scapular fracture that limits muscular dissection, can improve rehabilitation, and can limit morbidity of the operation.
|
|
|
|
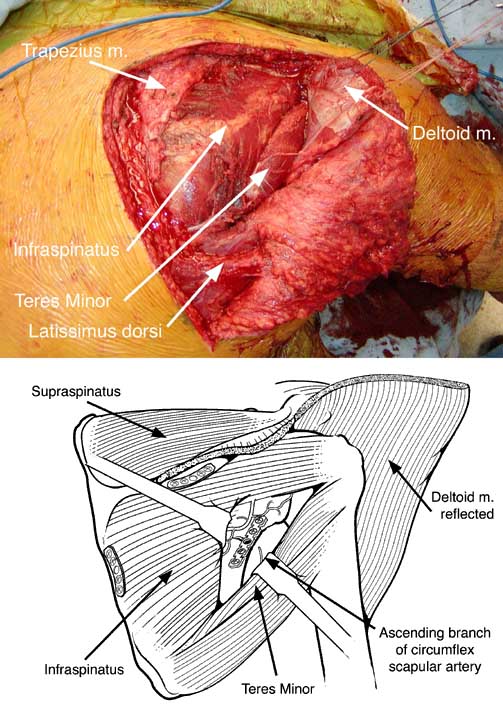
Methods: The patient is placed in a prone position with the ipsilateral arm draped free and a small bump placed under the anterior chest. The extensile skin incision as described by Judet is based on the subcutaneous border of the scapular spine and angled sharply at the superomedial angle of the scapula and follows the medial border inferiorly to the inferior angle. Sharp dissection to the fascia is performed. A large skin flap and associated subcutaneous fat is elevated off the fascia, exposing the infraspinatous, teres minor, teres major, and posterior deltoid muscles of the scapula. Scissor dissection with a curved Mayo in the areolar tissue plane facilitates this exposure better than electrocautery. The skin flap then is extended laterally beyond the lateral scapular border. The plane between the posterior deltoid and the infraspinatus muscles should be developed by use of blunt dissection. The fascia of the posterior deltoid is then dissected off the spine of the scapula, releasing the origin of the posterior deltoid. The posterior deltoid origin with the overlying fascia is tagged and retracted superolaterally. Laterally, the plane between the teres minor and infraspinatus muscles is developed and allows exposure of the ascending branch of the circumflex scapular artery, which is ligated. If this vessel is inadvertently cut, it may be a source of rapid bleeding, and vascular clips should be readily available.
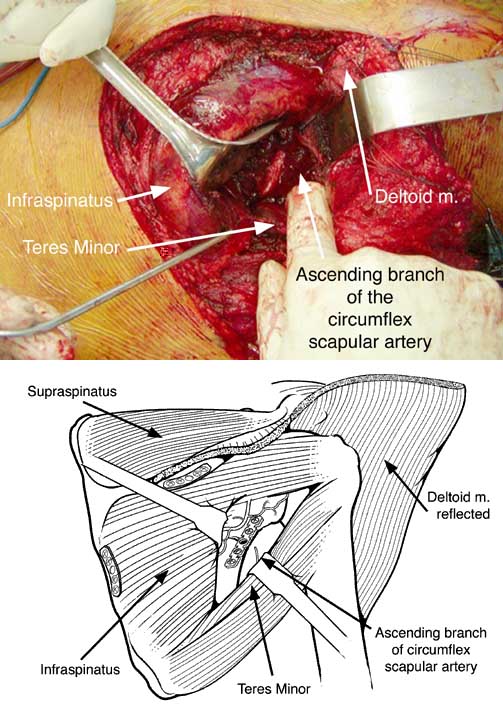
Careful retraction of the lateral portion of the teres minor and infraspinatus muscles allows exposure of the lateral border of the scapula (Figure 2 and 4). From this position, mobilization and reduction of the fragments may indirectly reduce a fracture of the glenoid surface and the glenoid neck. Mobilization, reduction, and fixation of these fractures can be difficult, especially if the fracture is approached 1 to 2 weeks after injury. Reduction can be facilitated by placement of k-wires or Schanz screws into the scapular lateral border, glenoid neck, or scapular spine. These can be used to mobilize and manipulate the fracture to improve reduction. Reduction can be held with small pointed reduction forceps or by applying a small external fixator to the Schanz screws. Pre-contouring and fixing the plate to the intact lateral scapular border can also aid reduction by allowing clamping of the plate to the short glenoid neck segment of the fracture. Glenoid neck fractures are commonly reported to be medialized. In the authors' experience, reduction of glenoid neck fractures usually requires medialization of the scapular body rather than lateralization of the glenoid. The deforming forces of the infraspinatus, subscapularis, and teres minor muscles pull the body laterally or reduction of a glenoid neck fracture requires medialization of the inferior spike of the fracture as the inferior aspect of the fracture has abducted away from the scapular body, or both may occur.
Buttress plating of the lateral border of the scapula with 2.7 or 3.5 mm reconstruction or DC plates or periarticular screws or both may be applied from this exposure (Figure 2). Some fracture patterns involve displacement of the scapular spine or medial border of the scapula, and these may be reduced directly with this exposure and stabilized with 1/3 tubular or reconstruction plates. Exposure of the medial spine may be done with minimal dissection and exposure only on the medial border of the scapula. Closure of the approach involves repair of the posterior deltoid muscle back to the scapular spine through drill holes with nonabsorbable suture and layered closure of the skin flap.
Results: Ten patients underwent this approach with anatomic reconstructions and no perioperative complications.
Conclusions: This exposure combines several important goals: 1) exposure of the bony elements of the scapula, which have adequate bone stock for internal fixation; 2) minimal trauma to the rotator cuff musculature; and 3) protection of the major neurologic structures (suprascapular nerve superiorly and axillary nerve laterally).
Significance: This approach can be used to allow accurate reduction of all scapular fractures with minimal morbidity.